The ophthalmologist will look for a wandering eye, as well as a difference in vision between the eyes or poor vision in both eyes. Depending on the child’s age, tests may include the following: * Newborns: Red reflex test to look for cataracts, using a lighted magnifying device (ophthalmoscope) * Infants: Test for ability to fixate their gaze and follow a moving object, as well as check for strabismus * Toddlers: Red reflex test, photo screening or remote auto refraction * Preschoolers and older children: Testing using pictures or letters. Each eye is patched in turn to test the other The doctor may also check for inflammation, tumors and other inner eye problems. Common causes of the condition
Muscle imbalance (Squint): The most common cause of lazy eye is an imbalance in the muscles that position the eyes. This imbalance can cause the eyes to cross in or turn out, and prevents them from tracking together in a coordinated way.
Difference in sharpness of vision between the eyes (refractive anisometropia): A significant difference between the prescriptions in each eye can result in lazy eye. Glasses or contact lenses are typically used to correct these refractive problems.
Deprivation of sight: Any problem with one eye — such as a cloudy area in the lens (cataract) — can deprive a child of clear vision in that eye. Deprivation amblyopia in infancy requires urgent treatment to prevent permanent vision loss. Deprivation amblyopia often results in the most severe amblyopia.
Treatment options depend on the cause of lazy eye and on how much the condition is affecting the child’s vision.
Corrective eyewear: Glasses or contact lenses can correct problems such as nearsightedness, farsightedness or astigmatism that result in lazy eye.
Eye patches: To stimulate the weaker eye, your child may wear an eye patch over the stronger eye. The patch is generally worn for two to six hours a day.
Eyedrops: A twice-weekly eyedrop of a medication called atropine (Isopto Atropine) can temporarily blur vision in the stronger eye. This will encourage your child to use the weaker eye, and offers an alternative to wearing a patch. Side effects include sensitivity to light.
Surgery: If the child’s eyes cross or wander apart, the doctor may recommend surgical repair for the eye muscles. The child may also need surgery if he or she has droopy eyelids or cataracts.
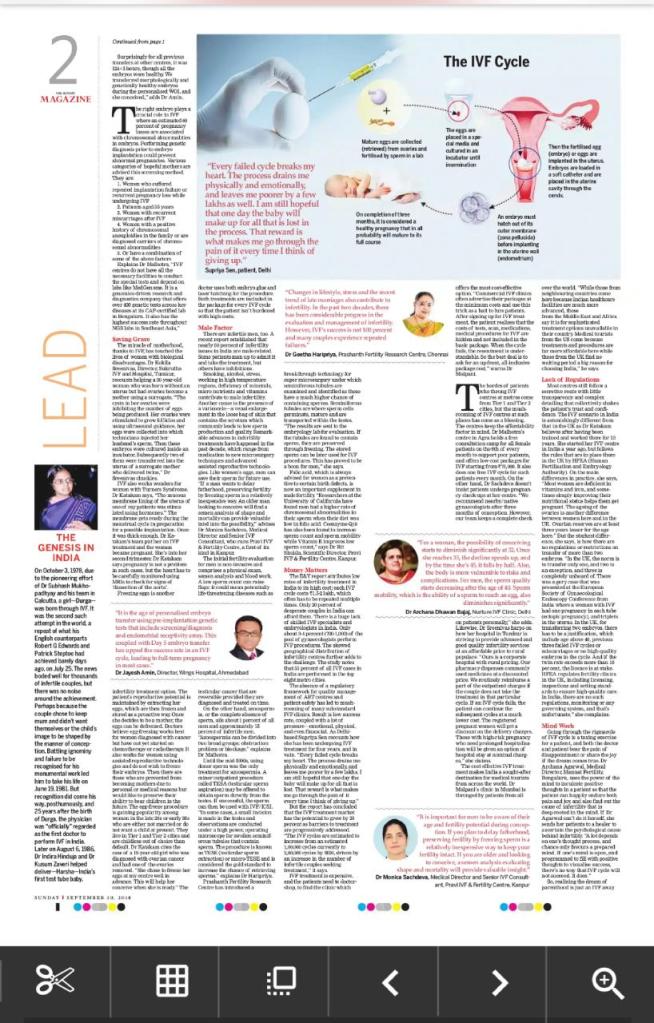
On October 3, 1978, Dr Subhash Mukhopadhyay’s and his team in Calcutta successfully delivered happiness in the lives of a childless couple with the birth of their little bundle of joy. The girl who was nicknamed Durga after the Hindu goddess was born through in-vitro fertilisation (IVF) thanks to Dr Mukhopadhyay’s pioneering effort that was the second such successful attempt for IVF across the world. It was a repeat of what his English counterparts Robert G Edwards and Patrick Steptoe had achieved barely days ago, on July 25 with the birth of Louise Brown, the world’s first such baby. The news bode well for thousands of infertile couples who yearned to become parents, but unlike the much celebrated IVF birth in England, there was no noise around his pioneering achievement, the first of its kind in India. Perhaps because the couple chose to remain mum and didn’t want themselves or the child’s public image to be shaped by the manner of conception, and the other stakeholders too remained indifferent to his remarkable achievement. Battling ignominy and failure to be recognised for his monumental work led him to take his life on June 19, 1981.
Meanwhile, Dr Indira Hinduja and Dr Kusum Zaveri helped deliver a baby girl named Harsha on August 6, 1986, who went on to earn the pride of being India’s first test-tube baby. But recognition did come Dr Mukhopadhyay’s way, posthumously, and 25 years after the birth of Durga, the Indian physician was “officially” regarded as the first doctor to perform in-vitro fertilization in India. The case in point explains the burden of having a progeny, often weighed down by the shame and embarrassment of not having one without any medical intervention, and sets the tone for the problem called infertility, a condition that needs attention and like any other ailment, can be cured with proper treatment. To fulfil parenthood dream, one needs to get past the maze of ignorance to access medical care that often comes at a price, endure all the pain that is borne by the patient, and doctor in equal measure, and get assurance in abundance that one day it would be all worth it with a baby around to wipe off all the weariness of undertaking the arduous journey called IVF.
Pandemic has forced the famous Cheriyal artists of Telangana to live in penury.
The handful of artists belonging to the Nakash caste and hailing from Cheriyal village in Telangana are the keepers of the visual form of storytelling popularly named after them as Nakashi art or Cheriyal paintings. Over the years, these artists have painstakingly preserved the rich cultural tradition of using pictures to tell stories from Indian mythology and local folklore. The proponents of this art form are heavily dependent on their art for survival, but the 15-month lockdown left them in the throws of woes.
The award-winning Nakashi artistsD Vaikuntam and his wife Vanaja.
“The Cheriyal art is on the brink of extinction. Today, only seven families are engaged in this art form. Five of these belong to the Nakashi community, and the others are outsiders who learned it from my father, D Vaikuntam,” says D. Rakesh, a young Nakashi artist. With no other source of income, his family of five – father Vaikuntam, mother Vanaja, brother Vinay Kumar, and wife Monisha – took to online workshops to fend for themselves during this period. The workshops conducted by SkillXn, Paramparik Karigar, Crafts Council of Telangana, Spic Macay, Dastkaar Haat Samiti, and Rajasthani Studios were creatively satisfying monetarily rewarding for his family. “The response was heartening, and the students showed keen interest in learning the art form. We want to keep it alive, and efforts like these will help us reach out to a wider audience,” says Vaikuntam.
The dying art form received a Geographical Indication status in 2007. Reminiscing the rich cultural tradition, Vaikuntam says, “Cheriyal scroll painting is one of the earliest forms of audio-visual entertainment. Hundreds of years ago, the storytelling communities travelled through villages, singing and narrating stories using the scroll as a visual tool. Each scroll measured about three feet in width and could extend to over 60 feet. A scroll contained about 40 to 50 panels, and each panel depicted a part of the story. These were displayed in a sequence to tell the tale.”
With newer forms of storytelling ruling the public imagination, the Nakashi artists have adopted unique ways to reinvent the art form and keep it relevant. “The pictorial tale from the epics doesn’t excite people anymore. The scrolls have been reduced to an aesthetic item adorning the walls, collected by art lovers,” rues Vaikuntam. To make the art form saleable, Nakash artists have designed utility items. “We made masks during the lockdown and sold them through our Facebook and Insta pages. We also use the traditional art form to make key chains, pen holders, and wall decor items,” says Rakesh.
Each Cheriyal scroll starts with a panel of Ganapati, followed by Goddess Saraswati. “It is customary for the artist to seek the blessing of the deities to ensure that the art flourishes without any obstacle,” says Vaikuntam. The Cheriyal scroll painting is drawn on handmade khadi cloth or canvas processed by applying a paste of tamarind seed, tree gum and white clay. Three coats of the paste are applied, allowing a day in between for the paste to dry. Once the scroll is ready, the artist outlines characters using a squirrel-haired brush. In Cheriyal scrolls, only natural colours are used like white comes from grounded sea shells, black from lamp soot, yellow from Pevidi stone, blue from Indigo leafs, red from Inglikam stone and the other colours from various vegetable dyes and ground stones. Every colour is mixed with thirumani tree gum, before being applied on the scroll. “The red colour fills the background. The face and skin colours are decided by the nature of the character, like blue and yellow are for gods and goddesses, respectively; brown or darker shades for demons, while pink and skin tones are for humans,” explains Vaikuntam. Text by Shillpi A Singh and photographs by P Mohanaiah and Tejaswini Paladi.
National Award winner Cheriyal artist D Vaikuntam.
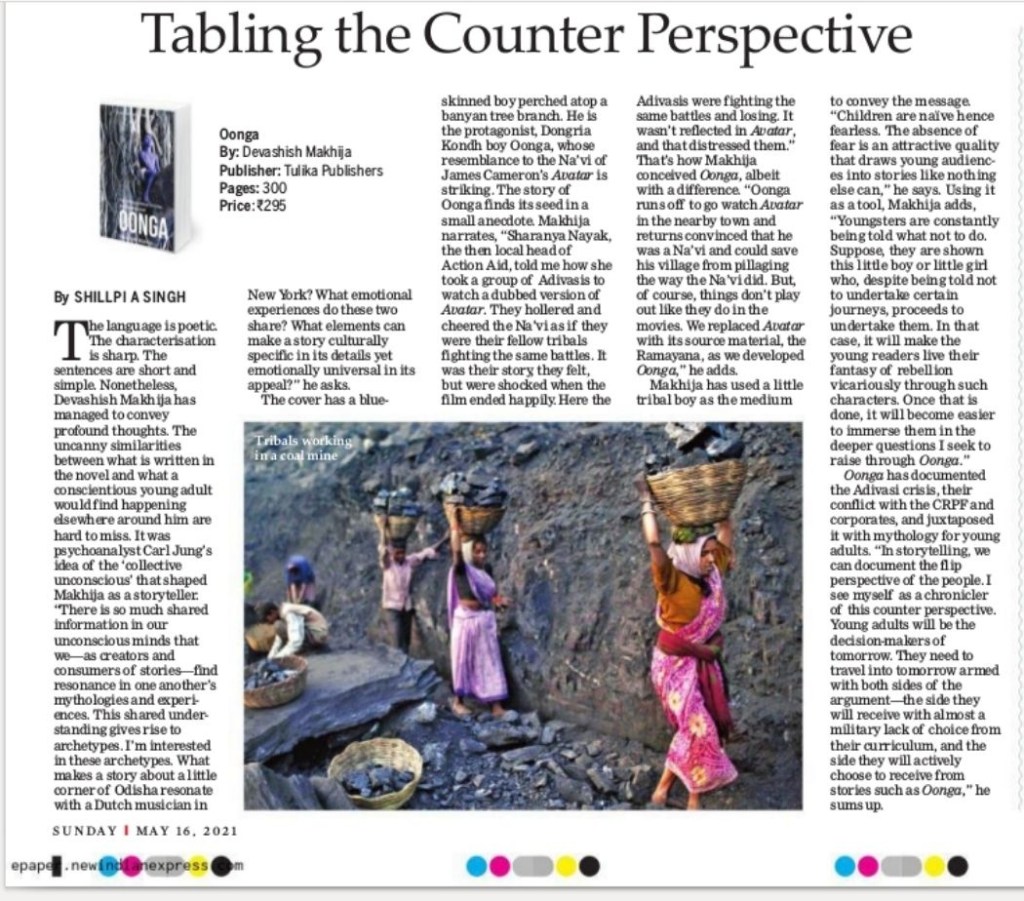
Writer-filmmaker Devashish Makhija’s critically acclaimed film Oonga has been reverse-adapted into a novel for young adults. Published by Tulika Books, it was released at the 14th Jaipur Literature Festival.
Q 1.The blue-skinned Dongria Kondh boy, Oonga, resembles the Na’vi of James Cameron’s Avatar. What is the back story?
Devashish Makhija (DM): The story of Oonga finds its seed in a small anecdote I heard while in Koraput, Orissa. Sharanya Nayak, the local head of Action Aid, told me how she had taken a group of Adivasis to watch a dubbed version of Avatar. They hollered and cheered the Na’vi right through the film as if they were their own fellow tribals fighting the same battles they were. They felt like it was their own story being shown on that screen. But they were shocked when the film ended. It ended ‘happily’! Though many years later, the group of Adivasis were still fighting the same battles and losing. Something about that not being reflected in Avatar distressed them. When we conceived the story of Oonga, he was to run off to watch Avatar in the nearby town, and return convinced that he was a ‘Na’vi’ and could save his village from pillaging the way the Na’vi did. But, of course, things don’t play out in the real world like they do in the movies. We replaced Avatar with its source material, the Ramayana, as we developed the story further.
Q 2.What was your most crucial literary tool for reaching out to young readers?
DM: Swiss psychoanalyst Carl Jung’s idea of the ‘collective unconscious’ has perhaps shaped me as a storyteller. As Jung’s words suggest, there is so much shared information in all our unconscious minds that we – as creators and consumers of stories – find resonance in one another’s mythologies and experiences. This shared understanding gives rise to archetypes. Like most storytellers, I’m very interested in these archetypes, in what makes a story about a little corner of Orissa resonate with a Dutch musician in New York. What emotional experiences do these two share? Hence, what elements can make a story culturally specific in its details yet emotionally universal in its appeal?
Q 3.How was it documenting the Adivasi crisis and their conflict with the corporates, juxtaposing it with mythology, and presenting it for young adults?
DM: Stories are the ‘people’s perspective’. The people cannot write history books. Those in power do. And history books end up being the primary source of information of our times for future generations. It is dangerous that any other perspective but the ruling regime’s is always missing from the history books – since time immemorial. In storytelling, we can document the flip perspective of the people… of those being marginalised. I see myself as a chronicler of this counter-perspective before I see myself as a storyteller even. Young adults will be the decision-makers of tomorrow. And I need them to travel into tomorrow armed with both sides of the argument – the side they will receive with almost a military lack of choice from their curriculum; and the side they will actively choose to receive from stories like Oonga, outside their curriculum.
Q 4.Using a 10-11-year-old tribal boy as the medium to convey the more prominent and more pertinent message to young adults. Why is he not an adult?
DM: Children are naïve hence fearless. If you don’t know, something can hurt you that something won’t scare you. And the absence of fear is a very attractive quality that draws young audiences into stories like nothing else can. Youngsters are constantly being told what NOT to do. If, suddenly, they are shown this little boy or little girl who, despite being told NOT to undertake certain journeys, proceed to undertake them, the youngsters reading the story love to live their own fantasy of rebellion out vicariously through such characters. Once that is achieved, once I have reeled them in, I can then slowly immerse them in the deeper questions I seek to raise through the story.
The Iranian cinema of the 1980s and 1990s did this successfully. Oonga is me trying to attempt that.
Q 5.What are the similarities and differences in your writing process when you chose to pen a novel for young adults (vis-à-vis children’s books and short and feature films)?
DM: A novel is a gargantuan beast.
In a short story, a children’s picture book or a short film, I don’t have the liberty of character establishment. I often need to get into the thick of the action almost as soon as the story begins. Also, a short story cannot ‘end’ in a conventional way. Closing the loop neatly in a short story is almost impossible given how little time we’ve spent with the characters. It becomes very important there to choose very carefully the ‘portion’ of the characters’ journey I want to make the story about.
The other thing this allows for then in the shorter mediums – short story, children’s book, short film – is multiple revisits by the reader/viewer. A short story or children’s book could be like a favourite song that you can play again and again. A novel demands much more time and attention and investment to provide this kind of a relationship with the reader.
I consciously approach a shorter format story in a way that the narrative doesn’t close its loop by the end. Questions stay unanswered. Characters stay partially undiscovered. The story feels like it could go on.
But with a novel like Oonga each character has his/her own complete arc, even as the story has one of its own. I map each arc beforehand, so I know their intersectionalities, convergences, and divergences before starting the physical writing process. The abruptness of a wildly open-end can leave the reader very dissatisfied in a novel because I have drawn them into a ‘world’ that they inhabit with the characters for over 300 pages.
Whereas the shorter storytelling forms allow me to undertake more of an exploratory creative process, a novel needs all the engineering, cartography, universe-building skills I can muster. Whereas the shorter forms end up mostly being about the character(s), a novel like Oonga needs to be about a well-charted story, an amply-detailed universe, as well as deeply-plumbed characters.
The mind, the heart and the eye need to be prepared differently for both.
Q 6.Dialogue is one of the most important themes that you have touched upon in this book. How do you think this novel can help start a conversation around the issues that you have spoken about in Oonga? What are your expectations from this novel?
DM: There are some things in life we don’t think about often and deeply enough. Our daily lives always get in the way. Death, Injustice, our Anthropocentrism, our capacity for Hate, our very imbalanced view of Development… I like raising questions about these through my stories. Generally, I never have a solution or an answer. I simply share with the viewer my own heartburn, hoping that these questions will haunt them once they emerge from my stories, and keep asking them too.
Q 7.Do you think a socio-political writer or artist can bring about a real tangible change in society?
DM: No idea. Of course, all of us harbour delusions of grandeur, hoping to affect people enough to get them to question the status quo in more significant numbers to effect social, political, anthropological change. We see dreams of this happening when we write our stories and create our art. But can an artist or a storyteller achieve that? Like a policymaker or political leader can? Who knows. I’m not holding my breath for it.
All I can say for sure is that I create my work this way because if I didn’t put my unrest and heartache and rage and questions and protest into my stories, I’d self-destruct. I do this so I can get some sleep at night, however, disturbed.
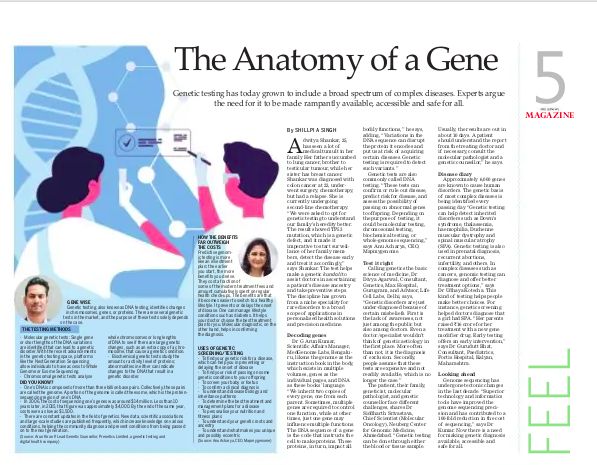
Genetic testing has grown from a niche speciality for rare disorders to a broad scope of applications for routine, complex diseases to its use in personalised health solutions and precision medicine. There is a need for healthcare providers, the diagnostic community and the government to step-up and uplift genetic diagnostics, making it available, accessible and safe for all.
Dr G. Arun Kumar, Scientific Affairs Manager, MedGenome Labs
Dr G. Arun Kumar, Scientific Affairs Manager, MedGenome Labs.
Explain genetic testing/screening to a layman. What are the challenges of genetic testing?
To understand genetic testing, it is essential to understand the role of DNA and genes in our bodies. We can see our genome as the instruction book in our body which exists in multiple volumes, the genes as the individual pages present in these books, while the DNA is the language in which the pages are written. Genes regulate specific parts or functions of a cell. We inherit two copies of every gene, one from each parent. Sometimes multiple genes are required to control one function. Other times, just one gene may influence multiple functions. The DNA sequence of a gene is the code that instructs the cell to make proteins. These proteins, in turn, affect all bodily functions. Any variations in the DNA sequence can disrupt the protein it encodes and put us at greater risk of acquiring certain diseases in our lives. Genetic testing is a tool used to look at our DNA to detect such variants. Results from a genetic test can significantly help doctors understand the cause of a disease or symptoms, predict an individual’s risk of developing certain diseases, tell if one could pass the disease to their children and help in choosing the best treatment that can be tailored for the individual. For instance, if a person has cancer, then a genetic test can tell if the person inherited a cancer-causing genetic aberration. Early detection can also help doctors make an informed decision about the same and tell if the patient is at risk of developing any other type of cancers as well. Genetic testing of cancer tissue can help in identifying genetic variants that can be targeted using specific drugs.
Performing genetic testing requires high expertise both in terms of laboratory testing and analysis of genetic data. Understanding a genetic testing report for a commoner requires a clinician or a genetic counsellor.
If I have hereditary spherocytosis, can I get to know the chances of it being carried by my offspring and how?
In most cases, spherocytosis occurs as an inherited disease that changes and reduces the life of red blood cells in the patient’s body and causes anaemia. The initial evaluation of hereditary Spherocytosis involves a physical inspection, a review of the family history, and few lab tests on blood samples. In Spherocytosis, the structure of red blood cell changes, attributable to a defective protein produced in the cell due to genetic mutations. Genetic testing for spherocytosis looks for variants in the genes ANK1, EPB42, SLC4A1, SPTA1, SPTB. Some of these genetic variants are inherited in an “Autosomal recessive” manner. It means that for a person to express the disease (s)he must inherit genetic variants in both the gene’s copies. If a person has inherited a genetic variant in only one copy of the gene, the other copy being healthy, then this person is termed as a carrier. A person with the disease will 100% pass on one defective copy of the gene to the offspring. On the other hand, an individual who is a carrier has a 50% chance of passing the offspring’s variant. In either case, if the partner of the individual also passes on one defective copy to the offspring, then the child will develop the disease.
What are the things to keep in mind while opting for genetic testing/screening? What are its hope for medical science in the days to come?
Genetic testing can help in identifying an inherited disease risk in an individual. It is important to discuss the reasons for a genetic test with your doctor as they may guide you to a medical geneticist who is trained to diagnose a genetic condition, select the appropriate genetic tests, explain the test results, and recommend personalized treatment and prevention options. Before opting for genetic testing, one should gather as much information as possible about the family’s medical history to understand the risk better.
What are the diseases for which this screening works?
MedGenome currently offers more than 475 genetic tests across several disease categories such as paediatrics, neurology, oncology, haematology, endocrinology, nephrology, ophthalmology, etc. Any disorder that has an established genetic basis can be screened. Additionally, we also offer carrier screening for couples that will tell the carrier status of various genetic variants in the couple. This shall aid the clinician counsel the couple for future pregnancy.
What are the services offered by MedGenome?
Medgenome offers genetic testing services under four major divisions, viz – Actia, Claria, Prima and Micra. The Actia division deals with genetic testing of all inherited disorders encompassing all major medicine disciplines, including neurology, ophthalmology, cardio-vascular, Metabolic disorder, Nephrology, etc. The Claria division deals with reproductive genetics that offers various prenatal genetic testing panels, NIPT, and pre-implementation genetic testing. The Prima division deals with Oncology (solid tumours and Leukaemia) and Hematology range of testing. All these tests are College of American Pathology accredited. The Micra division is a new addition to our portfolio that is involved in infectious disease testing. In this range, we have indigenously developed the first whole genome sequencing of Mycobacterium tuberculosis directly from a patient’s sputum.
MedGenome is the market leader in India’s genetic diagnostics and is one of the largest high- throughput NGS sequencing labs in South Asia. We possess state-of-the-art Next-generation Sequencing (NGS) facility, which houses cutting-edge genome sequencing platforms such as Illumina’s NovaSeq, HiSeq X, HiSeq 4000 and 2500, MiSeq, etc. A sophisticated IHC pathology lab supports our Sequencing facility. We also offer other genomic testing technologies such as FISH, PCR, Sanger Sequencing, and Microarray to offer comprehensive diagnostic solutions to clinicians, hospitals and researchers. We offer genetic testing at different scales such as identification of point mutations using Sanger technique, RT-PCR; chromosomal level aberrations using FISH, Chromosomal microarray; multigene and whole-genome sequencing using Next Generation Sequencing
Is genetic testing gaining popularity?
Genetic testing is gaining popularity among all medicine disciplines because of its wide applications inpatient management and family planning. Almost all significant guidelines of different medical disciplines have incorporated genetic testing in their statements. The awareness of genetic testing among the general public is also increasing so much so that direct consumer testing for personal genomics is not far from reality.
What are the cost implications?
Genome sequencing technology has undergone tectonic changes in the last decade. The development of superior technology and informatics tools has improved genome sequencing precision and has contributed to a 100-fold reduction in sequencing cost. MedGenome has been a forerunner in India for democratising genome sequencing by making it affordable, beyond the reach of a commoner a decade ago, without compromising the quality.
Arun Kiran P, Lead Genetic Counsellor, Prenetics Limited
Arun Kiran P, Lead Genetic Counsellor, Prenetics Limited.
Explain genetic testing?
Genetic testing, also known as DNA testing, is a process of identifying changes in chromosomes, genes, or proteins.
Genetic testing results can help individuals either confirm or rule out the possibility of having a clinical condition; identifying genetic mutations can determine a person’s chance of developing genetic predisposition risk or passing on a genetic disorder.
There are several genetic tests in the market, and the purpose of these tests solely depends on the case and the scenario it is in use. Several methods are used for genetic testing:
Molecular genetic tests: where single genes or short lengths of the DNA variations are identified that can lead to a genetic disorder. With the recent advancements in the genetic testing space, platforms like the Next Generation Sequencing allow individuals to access Whole Genome or Exome Sequencing (WES).
One’s DNA is composed of more than 3 billion base pairs. Collectively, these pairs are called the genome. A portion of the genome is called the exome, the protein-sequencing region of one’s DNA.
Chromosomal genetic tests analyse whole chromosomes or long lengths of DNA to see if there are large genetic changes, such as an extra copy of a chromosome, that cause a genetic condition.
Biochemical genetic tests study the amount or activity level of proteins; abnormalities in either can indicate changes to the DNA that result in a genetic disorder.
2) If I have hereditary spherocytosis, can I get to know the chances of it being carried by my offspring and how?
Hereditary spherocytosis is a condition characterized by haemolytic anaemia (when red blood cells are destroyed earlier than normal).
Signs and symptoms can range from mild to severe and may include anaemia, pale skin, fatigue, jaundice, gallstones, and/or enlargement of the spleen. Severe cases involve short stature, delayed puberty and skeletal abnormalities.
Mutations cause this condition in any of the several genes, such as the ANK1, EPB42, SLC4A1, SPTA1, and SPTB genes. It is most commonly inherited in an autosomal dominant manner but may be inherited in an autosomal recessive manner in rare cases. Different types of hereditary spherocytosis are distinguished by severity and genetic cause.
Autosomal Dominant Inheritance:
About 75% of cases of hereditary spherocytosis are inherited in an autosomal dominant manner. This means that having a change (mutation) in only one copy of the responsible gene in each cell is enough to cause the condition.
When a person with a mutation passes on to the child for an autosomal dominant condition, each child has a 50% (1 in 2) chance to inherit that mutation.
In rare cases, hereditary spherocytosis is inherited in an autosomal recessive manner.
A person must have inherited one mutated gene copy from each parent, who are referred to as genetic carriers.
When 2 carriers of an autosomal recessive condition have children, each child has a:
– 25% (1 in 4) chance to be affected
– 50% (1 in 2) chance to be an unaffected carrier like each parent
– 25% chance to be unaffected and not be a carrier
Carriers of an autosomal recessive condition typically do not have any signs or symptoms (they are unaffected). By doing a full gene analysis of these genes, one can understand the risk of passing it on to their offspring.
Any interesting case study or success story?
Ms Roopa, who is in her early 30s from Bangalore, reached out to me as she had a strong family history of breast cancer on the maternal side of the family. Ms Roopa’s mother and maternal aunt were diagnosed with breast cancer in their 40s and she was very worried about her potential risk of being diagnosed with Breast Cancer in future. As a genetic counsellor, I explained to Ms Roopa about the potential chances of inheriting a genetic mutation in one of the cancer-causing genes associated with breast cancer based on the family history she had described.
Ms Roopa was suggested to get her mother tested for a hereditary cancer panel consisting of breast cancer-causing genes. Based on the hereditary breast cancer panel analysis, it was found that Ms Roopa’s mother had a genetic mutation in PALB2 gene, which is strongly associated with Breast cancer, and this mutation is also known to increase the risk of pancreatic cancer and ovarian cancer.
The genetic mutation that was detected in Ms Roopa’s mother was tested for Ms Roopa and based on the analysis the same genetic mutation was inherited in the PALB2 gene. This led to an understanding that Ms Roopa has an increased risk for the above-mentioned hereditary cancer conditions.
As the genetic mutation present in the gene PALB2 follows an autosomal dominant mode of inheritance where there is 50% chance for the genetic mutation to be passed on to the offspring. Based on these interpretations and findings, specific screening and surveillance measures were suggested to Ms Roopa based on the National Comprehensive Cancer Network® (NCCN®). Due to the genetic mutation being present the surveillance and screening needs to start as early as the age of 30 onwards considering the family history and clinical data.
Ms Roopa was suggested to do Annual mammography with consideration of tomosynthesis along with consideration of annual breast MRI with contrast starting at age 30, with modification as appropriate based on family history by discussing with the physician.
Potential management options such as prophylactic risk-reducing mastectomy (surgery to remove one or both breasts to reduce the risk of developing breast cancer by up to 95%) was suggested as an option by having a discussion with the oncologist based on the family history.
Knowing if a PALB2 genetic mutation is present is advantageous. At-risk relatives, i.e., first/second-degree relatives, can be identified, enabling the pursuit of a diagnostic evaluation.
Getting the genetic test done has helped Ms Roopa be more proactive about her health and do these screenings from an early age onwards to help in potentially detecting any breast cancer tumours at the early stage of cancer for better treatment management purposes as most of the cancers do not show immediate symptoms and go undiagnosed till late stage of cancer-causing lesser chances of survival.
As a genetic counsellor, all the questions related to risk assessment, limitations of the genetic test, screening and surveillance options, and management options were discussed with Ms Roopa by giving her access to the right set of resources and a specialised doctor who can help her with overall process. More insights were provided based on the genetic findings to Ms Roopa and she was able to take her own choice based on the options provided by the genetic counsellor and the physician.
What are the things to keep in mind while opting for genetic testing/screening? What is its hope for medical science in the days to come?
Every genetic test is performed based on the situation. Individuals need to talk with their physician, geneticist or genetic counsellor to have a better understanding, especially when it comes to a diagnosis or a clinical condition.
There are things to keep in mind before deciding on a genetic test. Such as the test platform, test limitations, laboratory accreditations, measures taken to safeguard data and privacy, ability to access raw data. And most importantly, having access to genetic counsellors to understand the results to avoid undue stress and misinterpretation.
Accessibility of genetic tests has been dramatically increasing, and prices are still dropping to this day.
In 2006, the cost of sequencing one’s genes dropped to around $14 million. Less than ten years later, in 2015, that figure dropped to approximately $4,000. By the end of the same year, costs were as low as $1,500.
There are constant updates in the field of genetics. This means new data, scientific associations and massive large-scale studies are published frequently, which increases knowledge on various conditions. This indeed helps the community diagnose and prevent conditions from being passed on to the next generation.
Due to an increase in budget for research and development in the field of medical sciences, drug discovery and gene-therapies will be available for many rare conditions. This includes common health conditions that leads to personalised health solutions and precision medicine.
What are the services offered by Prenetics Ltd and what are the cost implications?
Depending on which CircleDNA kit one chooses, we provide different sets of information.
Vital kit (HK$1,192 ~ 11k INR) includes reports across 14 categories centring on diet, nutrition, fitness and overall wellness
Health kit (HK$3,192 ~ 30k INR) includes reports in four categories looking at health risks such as cancer and disease
Family Planning kit (HK$3,192 ~ 30k INR), made for those planning to conceive, is focused on the assessment of your carrier status for hereditary conditions.
Premium kit (HK3,992 ~ 37k INR) is the most comprehensive genetic test in the market, which offers more than 500+ reports across all categories.
Note that the CircleDNA results are not medical advice or report. They should not be used for diagnostic purposes. These tests are strictly meant to help individuals understand their genetic predispositions, where the results can be used to personalise their recommendations for optimum health.
What are the numbers like? Is it popular or gaining popularity?
The CircleDNA direct-to-consumer test under Prenetics Ltd has been quite popular in Asia, South East Asia, UK and in European countries.
On an average the lab processes more than 15,000 samples per month.
What is the turnaround time for the test?
From the sample collection to the test results being ready in the CircleDNA app, the process takes around 3-4 weeks of time. The testing process is very simple. Using a cheek swab in the DNA collection kit, collect a saliva sample and send your sample back to the lab.
What are the diseases for which this screening works?
CircleDNA is a comprehensive genetic test which consists of 500+ reports and tests for categories like Diet and Nutrition, Well-Being, Stress and Sleep, Pollution, Skin, Talents and Sports, Sports and Fitness, Success Traits, Music and Dance, Ancestry Test Results (with up to 15 geographical categories), Personality Traits, Behavioural Traits, Physical Traits, Gender Traits, Carrier Screening for understanding the risk of passing on the risk to the child (Family Planning), Hereditary Cancer risk.
The test helps an individual understand if h/she has inherited any mutation, increasing the risk for Cancers with a genetic basis, Dementia & Brain Health, common health risks such as obesity, stroke, and type 2 diabetes. Such health risks are very prevalent among the South Asian population.
Dr Gurudutt Bhat, Consultant – Paediatrics, Fortis Hospital, Kalyan
Dr Gurudutt Bhat, Consultant – Paediatrics, Fortis Hospital, Kalyan.
What are the opportunities and challenges of genetic testing?
The COVID19 pandemic has truly showcased India’s medical engineering talent, scientific expertise and the country’s potential to become a healthcare hub of the future. In this growth story, what stands out is India’s vast opportunity to achieve dramatic improvements in health outcomes. One way to that is genetic testing. Genetic testing has come a long way in preventive medicine, especially among pregnant women and their babies.
Blood and other tests are done mainly in pregnant women to rule out any diseases caused by a defect in the baby’s genes. It helps the expectant mother and her treating Obstetrician to manage the pregnancy and delivery appropriately. Some of the defects which can be detected are of the baby’s brain or spine etc. It can be an invasive test like a blood test or Amniotic Fluid Test, or non-invasive test like Ultrasonography. After the baby is born, its genetic sequencing can help confirm any gene mutations’ presence or absence. If the family already has an older child with genetic disorders, this test will help the subsequent baby be diagnosed early, and appropriate intervention can be initiated.
A great example of genetic screening is in older women who get pregnant after the age of 34yrs. These women are at high risk of having babies with Down’s Syndrome. Since it is a genetic disorder, the early screening will help detect such defects. This allows the family understand the consequences of the defect. They can undergo appropriate counseling, and it also helps the mother deliver the baby with proper precautions.
The biggest challenge for the success of genetic testing in India is its high cost. However, with the increasing use of genetic screening in India, the cost factor is slowly balancing out. Another problem area is that like everything else in medicine, this is not an exact science. There is a lot of evidence that still needs to be organized. There may be some problems with the tests available with some genetic testing companies, and not all tests are available easily in India.
When does genetic disorder get transmitted from a mother to her baby?
The defects in a mother’s X chromosome can be inherited by both male and female babies. A defect in Y chromosome can only be detected in a male baby. A defect in the other chromosome can be transmitted to a baby in two forms known as autosomal dominant i.e. the gene will express dominantly in the baby even if there is only one copy of that gene on a chromosome. In an autosomal recessive genetic conditions both copies of the gene are needed for expression.
If I have hereditary spherocytosis, can I get to know its chances being carried by my daughter?
Hereditary spherocytosis is a genetic defect leading to a defect in the spectrin protein, which make the red blood cell membranes fragile. This red blood cell breakdown causes anemia and its complications. Up to 75 % of hereditary spherocytosis cases are autosomal dominant gene induced hence can be seen in babies of mothers with this condition. Hence, early diagnosis and proper treatment can prevent complications.
Any interesting case study or success story?
A recent case of a girl with the genetic problem of Spino-Muscular Atrophy can be a classic example of a success story. Due to genetic screening, doctors were able to diagnose her medical condition. Her parents raised Rs 16 crores for her treatment with a new gene modifier drug. This is a testimonial to the future where early genetic testing can help find a cure and offer early interventions for some genetic conditions.
What are the things to keep in mind while opting for genetic testing?
The idea for seeking genetic testing is to find way to prevent or treat certain conditions that we might be predisposed to. Decide which screening tests you need (to find a disease at an early stage when it might be more treatable), is important, so seek advice before testing:
Think about your reasons for wanting the test
Get the right tests
Ensure that you and your family are prepared for the results
Ensure that you have a personalized plan for dealing with the diagnosis
What is its hope for medical science in the days to come?
Genetic testing can help people make healthy choices. For instance, in a family that is predisposed to developing a certain kind of Colon Cancer or any other factors that can cause Cancer, genetic screening can help identify this risk. The opportunities this discipline offers for arriving at better health outcomes and personalized medicine are immense. We must realize that genetic testing has grown from a niche speciality for rare disorders to a broad scope of applications for routine, complex diseases and personal use. However, there is a need for healthcare providers, the diagnostic community and the government to step-up and uplift genetic diagnostics, making it available, accessible and safe for all.
Dr Udhaya Kotecha, Lead Clinical Geneticist, Neuberg Centre of Genomic Medicine
Dr Udhaya Kotecha, Lead Clinical Geneticist, Neuberg Centre of Genomic Medicine.
If I have hereditary spherocytosis, can I get to know its chances of being carried by my daughter?
Hereditary spherocytosis is a condition where hemolytic anemia occurs due to destruction of red blood cells. Currently, five genes are known to be causative for this disorder (genetic heterogeneity: where a single disease can be caused by genetic disease, causing variation in more than one gene). A patient suspected of having hereditary spherocytosis can have the same due to genetic variation in any one of the five genes. It is commonly inherited in an autosomal dominant manner, meaning that if one of your gene copies is carrying the variant, you may manifest symptoms. There is a 50% chance that each of your offspring may inherit the disease-causing variant in this inheritance pattern. Rarely hereditary spherocytosis is caused by recessive mutations: meaning that both copies of the gene need to be alerted to have the disease. If you have hereditary spherocytosis due to a recessive mutation, the chances that your children will be affected depends on your partner’s carrier status. If your partner is also carrier, a disease-causing variant in the same gene, then there is a 75% chance of your children being affected. If your partner does not carry any genetic alteration in the same gene, then all your children will only be carriers, but none will be affected.
Dr Siddharth Srivastava, Chief Scientist (Molecular Oncology), Neuberg Center for Genomic Medicine
Dr Siddharth Srivastava, Chief Scientist (Molecular Oncology), Neuberg Center for Genomic Medicine.
What are the challenges of genetic testing?
The patient, their family members, consulting clinician/ medical geneticist, molecular pathologist, and genetic counsellor have stakes in the successful resolution of the patient’s problem. Interestingly all of them face different sets of challenges. Finding the genetic basis of diseases is a matter of speciality doctors. The first challenge the patient faces is navigating their way from general practice to these centres that are usually located in cities or large towns. The rarefied set of specialists doctors are further split into sub-speciality. Doctors who understand genetic basis of cancers or that of cardiovascular disorders, inherited diseases etc. To get to the right doctor, often naïve patients have to go through a maze of trial and error.
A conclusive diagnosis of such disorders or disease can be made by using molecular techniques. A dialogue between the consulting doctor and molecular pathologist sets up where the molecular pathologist understands the patient’s clinical history and clinician’s question. Accordingly s/he selects right test using most appropriate technique. This is crucial as molecular tests are complex, running into weeks and they are also expensive. For most accurate reports, the molecular pathologist should get detailed and accurate patient history which helps them to correlate molecular data and write accurate interpretations which will have deep implications on patient management. Acquiring patient’s clinical history is a challenge.
A lot of the times, diagnosis of the patient has implications on the immediate family members such as children, siblings, children of siblings. During the time of diagnosis of the patient, the “at risk” family members may seem to be leading a normal life. They do not feel concerned about their own chances of getting the disease in later parts of their lives. Genetic counsellors face tremendous challenges by collecting data from various family members and discussing the risks and convincing them to take the test.
Any interesting case study or success story?
Genomic testing has made both detection of inherited disorders, as well as treatment of complex diseases such as cancer and there, are countless success stories. There was a person from Mumbai whose mother (70 years old) was detected with breast cancer (ER+Her2- type). An extremely sharp cancer doctor was treating her with hormone therapy. After three years of treatment, she relapsed. This means that she stopped responding to the hormone treatment and the tumour grew despite getting the therapy. The doctor discussed with us at Neuberg Center of Genomic Medicine, and based on the clinical history, we predicted that most likely a defect in either ESR1 gene or PIK3CA gene may have resulted in the patient no longer responding to the treatment. If the defect was indeed in ESR1 gene, the doctor could changer her therapy to a drug called fulvestrant, and if the defect were in PIK3CA gene, then the drug would have changed to Alpelisib (approved by US FDA). However, the problem got compounded as the patient moved out of Mumbai, and the amount of tumour tissue was less to perform the test. We resorted to another test call liquid biopsy, where a tube full of patient blood was collected from her home and shipped to our laboratory. Indeed we detected a defect in PIK3CA, and the patient is now doing very well on Alpelisib therapy.
Another instance was that of a 45 years old man from Nashik who had prostate cancer. Since he was diagnosed at a young age with cancer, the clinical doctor suspected it to run in the family. The doctor connected with us, and one of our genetic counsellor spoke with the patient at length to get a history of cancers in the extended family. Patient’s mother had breast cancer at the age of 55, and she had since passed away. Genetic counsellor converts entire patient’s family history into the pedigree chart. Defects in BRCA genes and BRCAness genes could be the reason for the patient’s prostate cancer. If true, the patient could become eligible for a drug called Olaparib, and it would then become imperative to test his 15-year-old daughter too. We collected patient’s blood and tested for BRCA and BRCAness genes. Indeed the patient came positive for BRCA mutation. While it brought cheer to him, he also got concerned for his daughter. We tested the daughter and several of his “at risk” first and second-degree relatives. While his daughter had no pathogenic BRCA mutation, and she was considered as normal as any individual, patient’s 30 years old sister was detected positive with the same BRCA mutation. Thus the clinical doctor has kept her on active surveillance while doing periodic mammogram and breast exams.
What are the things to keep in mind while opting for genetic testing? What are its hope for medical science in the days to come?
While opting for genetic testing, one should know that either the blood or tissue sample would be asked from the patient. I would advice patients to collect their tissue samples from pathology labs if ever their biopsy is done. Usually the tests takes more than ten days to give out the results. Patients should take time to understand their report from the treating doctor and, if necessary, call the molecular pathologist. The patient should provide the detailed family history to the genetic counsellors.
The genetic basis of most complex diseases is being identified every passing day. Identifying the genetic cause helps to detect “at risk family members” and helps find newer therapies for the patient to manage disease such as cancer.
What are the diseases for which it works?
Most inherited disorders such as Down’s syndrome, thalassemia/haemophilia, muscle dystrophy/spinal muscular atrophy can be detected using genetic testing. Genetic testing is also used in prenatal diagnosis, recurrent abortions, infertility, mental retardation. In complex diseases such as cancers, genomic testing can diagnose and give newer and better treatment options. Approximately, 6,000 genes are known to cause human disorders, and the same can be tested via different genetic tests. The rapid rate of gene discovery is increasing the number of diseases known on an almost daily basis.
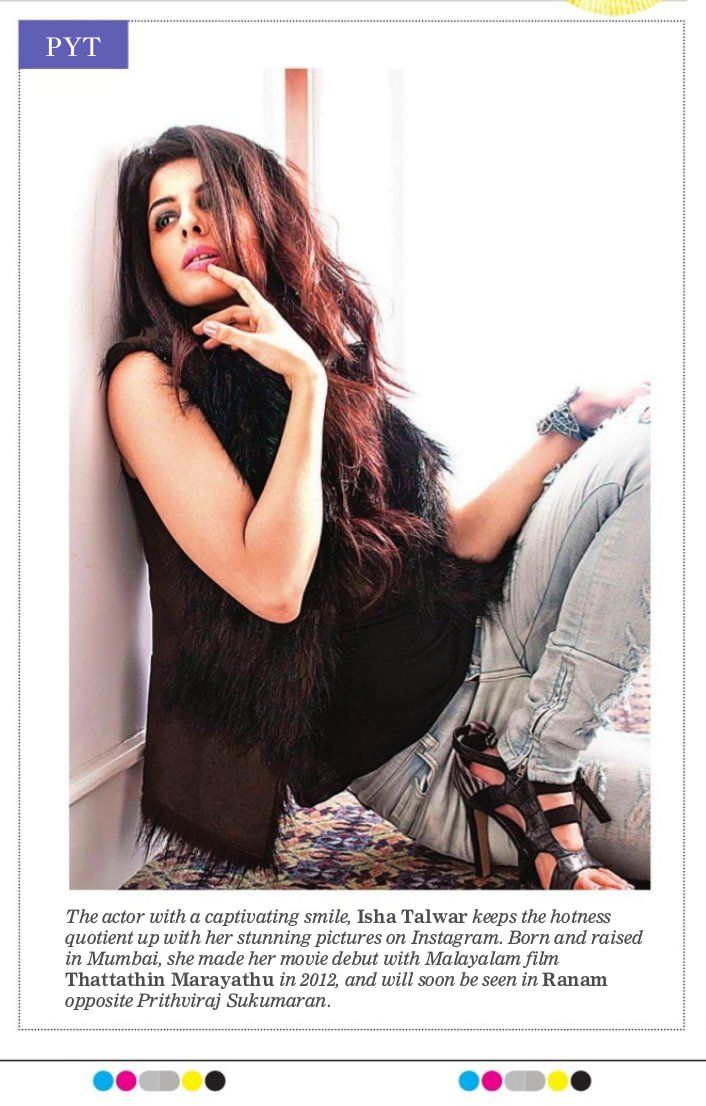
Born and raised in Mumbai, actor Isha Talwar landed in Kerala for an ad shoot, and her life changed altogether. She was spotted and cast in a Malayalam film, Thattathin Marayathu, in 2012. “It was a game changer, and opportunities came knocking from all over, and I was flooded with offers in Tamil, Telugu, and Malayalam,” she says.
Her next is an action flick, Ranam, starring Prithviraj Sukumaran to be directed by debutant Nirmal Sahadev where she plays mother to a 16-year-old. “Playing a mom to a teenage didn’t matter to me when I got a call, all that I asked was when and where do I have to come,” she says on bagging this role opposite Prithviraj. Having learned Malayalam, she’s moved bag and baggage to culturally vibrant Kochi because of work, and also because she loves everything about God’s own country. “I can go on and one about Kerala,” she chirps in, adding, “I would love to be the brand ambassador for Kerala tourism.”
Talwar made her Bollywood debut last year opposite Saif Ali Khan in the black comedy, Kaalakaandi and has a second film, tentatively titled Kaamyaab, by the makers of Masaan, alongside critically acclaimed actor, Sanjay Mishra.



















 .
.