क़लम मज़दूर | Commspreneur | Recipient of the IIMCAA Award for Public Relations Person of the Year 2024 | Canva's Top 10 Social Media Creator for 2023 | Work-in-Progress
View all posts by Shillpi A Singh →
Uttamchandani sibling trio – Ritesh, Shirley and Sonia.
Mumbai-based Uttamchandani sibling trio – Ritesh, Shirley and Sonia – had a rather sweet initiation into the home-grown food business with Sev Mithai or Singharji Mithai and Mohanthal, both traditional Sindhi desserts during the lockdown months. Ritesh was keen that Shirley become a home chef and start her business because the siblings were known for their Sindhi food among their friends and acquaintances. “It was always a super hit with everyone during the get-togethers but I was quite wary of log kya kahenge, especially the traditional Sindhis,” recounts Shirley.
Starting point
Ritesh wanted to share Sev Barfi with his friends on his birthday, and it was then that the idea first emerged. “It was around Ritesh’s birthday on July 30, 2020, that this idea first came up for discussion among us after one of his friends requested for it. We were thrilled to bits about the concept as we had received encouraging reviews from our friends to our food pop-ups. So we started the home delivery of mithais,” says Shirley. The trio was wary of people’s reaction, especially from the traditional Sindhis, but the sweet taste tickled their taste buds too, apart from finding favour among the non-Sindhis.
Sev Barfi.
“The response that we got was unbelievable! I was making big thals of Sev Barfi every day, not once or twice but even thrice. Every single person loved this flavourful sweet,” says Shirley. It tickled the taste buds of even the non-Sindhis. “Some of them were kind enough to heap praises by saying that it is better than Tharu’s at Bandra and Jhama Sweets at Chembur. Well, being even compared to these legendary sweet shops itself was a huge compliment,” says Sonia, adding, “Also, because we are using elaichi (cardamom) and kesar (saffron) generously.”
On the menu
Since then, their business has grown manifold, and they have had several additions to the menu, including traditional Sindhi foods such as Daal-Pakwan-Aloo Tikki, Sindhi Kadhi-rice-aalo tuk, Kokis, sanha pakoras, Sindhi mitha lolas, gajar ka halwa, Kaju barfi, seyal machi (fish), bhee alu,etc.
The culinary skill among the Uttamchandani siblings is hereditary. “My parents were wonderful cooks. Papa used to make finger-licking kadhi teevan (mutton) and fish till about he was 80. He always insisted on moderate use of spices so that the taste of vegetables retain its flavour. My mother used to cook amazing food. Her nieces and nephews settled abroad used to come and visit us because she used to pamper them with yummy chole kokis, sanha pakoras and mitha lolas and carrot and onion pickles made in Sindhi style,” says Sonia with a tinge of nostalgia.
Market wise
Sonia highlights how most of the upmarket eating places don’t have even Sindhi food added to their menu like south Indian, Punjabi or even Chinese, and that’s sad.
Ritesh attributes the rising popularity of Sindhi food among non-Sindhis to curiosity. “Over the years, our food culture has been influenced by other cuisines, and it has travelled to different parts of the world. It bodes well because, unlike the generation before mine that thinks it is diluting our culinary delights. I believe it is assimilation. Each Sindhi household has modified the dishes a bit, and still there’s a lot that remains the same,” he says. The Sev Mithai uses Sev as the main ingredient, and Sev is also used in the Kachchi dish, Sev Tamatar. Even Maharashtrians use Sev, so there are similarities, yet all the Sev dishes are different.
Their speciality is jaggery-based Sev Mithai. “Jaggery and milk are quite tricky to handle together but it’s Ritesh’s creative mind and the courage to experiment that has made this mithai a possibility and a success with those who don’t want to consume processed sugar. And this food experiment helped us even to make jaggery-based Mohanthal, which feels much lighter than the sugar version,” explains Shirley. Uttamchandani siblings have added orange-flavoured Sev Barfi as their next experiment.
Big takeaway
“Food has made possible such beautiful connections. People whom I have never met have become good friends of ours now. I am glad that our offerings have found a home in each of our client’s palate and plate,” chirps in Shirley, who can’t imagine how all of it started and how our food and sweets have so far reached more than 300 homes! “The connections that we have made are simply priceless. It is everyone’s love and God’s grace that has kept us motivated,” add Uttamchandanis.
Daal-Pakwan-Aloo Tikki
Sindhi Kadhi-Rice-Aalo Tuk
Capital Affair
Archana Manwani
Archana Manwani in the Capital loved to host non-Sindhi friends for lunches and dinners. “It was their encouragement that led to this food business. I take orders 24 hours prior because I prepare my food with specially sourced ingredients, be it vegetables or spices,” she says, adding that she learned traditional ways of cooking from her grandmother and mother-in-law.
Manwani, who is registered on mother’s food app, Sindhinama, and runs her business through a Facebook page, is quite keen to promote Sindhi cuisine among Delhiites.
“I approached Director of Tourism, Delhi Government, to allot a stall in Dilli Haat for promotion of Sindhi cuisine. We got no response from him even after two reminders.”
The FSSAI licensed home chef explains how Sindhi food is distinct in its typical preparation of food in sehal style (pan fried onion and tomatoes with vegetables like bhindi, baingan tinda, gobhi, etc). “Spices like jeera, sarson, khaskhas, amchoor, anardana and imli are quite common in our food,” she says.
Her special Sindhi dishes include:
Besni Bhaji: chickpea floor tillkis made in onions and khas khas deep fried and then sehal style.
Methi Meha Muthdiya: A traditional sindhi dish muthdiya made of wheat flour and steamed and the cooked with methi leaves and tinda.
Sai Bhaji/Bhuga Chawar/Took Patata; Kadhi Chawar; Sehal Bhaji Dhodho.
On special occasions, it is Dal Pakwan, Tikki Dabal Chola, and Seyoo Patata.
Sindhi home chef Archana Manwani.
Mother’s Delight
Poonam Shahani
Giving a rundown of how she got into the business, Mumbai-based home chef Poonam Shahani, who runs Mamma’s Cucina, says, “I used to cook for my family and friends of my children. Their compliments made me realise how so many of these dishes have never even been tried before. I started to realise that not many people are aware of what Sindhi food entails. And there’s a dearth of places that serve Sindhi food unless you visit one of the Sindhi camp areas in Mumbai.”
“Sindhi culture is getting lost somewhere. The younger generations don’t know how to cook Sindhi food. For the younger Sindhis, this food is like a piece of old memory served with love and platter. The flavour of my foods is clean and simple. I avoid using too much oil or ghee and customise spices according to a person’s taste. It reminds them of home and home-cooked food. The response has been great among non-Sindhis too! There is a Parsi man here who orders mutton and paya curry almost every other day.”
Sindhi food has a hint of Muslim influences, when it comes to our biryanis and mutton curries. This is because Muslim Sindhis and Hindu Sindhis lived together in pre-partition Sindh. In non-veg, the food in demand include Sindhi Mutton Basar Mein, Sayal Tewaran, Photewaro or Elaichi Kaare Mirchi Mein Mutton, Sindhi Paaya, Sindhi Mutton, Peas Keema, Sayal Green Masala Mein Machi while in veg, it is Sindhi Kadhi, Aaloo Took, Saibhaji, Toor Khati Daal, Dahi Curry, Bhi Aaloo Makwana ji Bhaji, Sindhi Veg Briyani Koki, and Daal Pakwan.
“I think it’s a mix of things. We use many vegetables that are nother otherwise found in other cuisines. We have a sabzi made of lotus stem called bhee aloo. We use drumsticks in Sindhi kadhi. We also use a technique to allow food to cook in its own juices called teewan. Teewan is essentially a gravy made of tomatoes, onions and spices. We make rice with it (seyal teewan), bread (seyal dabroti), roti (seyal mani) and mutton. We also prepare mutton curry with pepper and cardamom called Fote Bhugi Mutton,” says Shahani.
Mumbai-based home chef Poonam Shahani.
Chef Satyajit Kotwal of Satyajit’s Kitchen
Apart from having a unique flavour of its own, Sindhi food has an unmistakable mark of dynasties like Arabs and Mughal. The koftas biryanis and meat curries got infused into Sindhi cuisine during that time.
It’s different
They have a popular way of cooking Daagh, Seyal, Saye Masaley Main, and Dhaas, unique to their own culture. The distinction that sets it apart from other cuisines lies in cooking, which includes slow cooking technique, layering of herbs and spices with the right combination of sweet and savoury taste.
Chef’s favourite
Under vegetarian, my favourite would include Dhaas vegetables which are stuffed vegetables; it could be okra, apple gourds, capsicum, etc. Another one is Daagh which is a Sindhi curry prepared with brown onions. Seyal is another veg Sindhi breakfast prepared from leftover bread or rotis in a spicy or tangy curry-like gravy. Sindhi Kadhi is a unique and special dish prepared on festive occasions. It consists of a thick spicy gravy made from chickpea flour, unlike buttermilk, usually used for kadi preparation along with seasonal vegetables. Drinks that are famous with the Sindhis include thadal (made from almonds and poppy seeds), Khirni (hot drink made with milk, flavours of cardamoms and saffron), sharbat which is made from rose petals or sandalwood.
In non-veg, Bhuna Mutton is a famous Sindhi main course meal. Popular Sindhi biryanis and meat curries have a mix of flavor from the Arabs and Mughals. Pallo Machi is another popular Sindhi delicacy; it is Hilsa fish prepared with numerous cooking methods. It can be deep fried and garnished with local spices, can be cooked with onions and potatoes into a traditional fish meal or barbequed.
Different methods of Sindhi food preparations:
Sindhi foods are simple, and the flavour of vegetables is retained due to the minimum use of spices. Most common type of Sindhi cooking is Daag Mein, which is onion-tomato-based-curries. This method brings out the sweetness of caramelised onions to provide a balanced flavour to the curries. Another way of cooking is called Seyal where the amount of onions are added more than that of vegetables. The sliced or diced onions are cooked till translucent.
Saye Masale Mein is a Sindhi way of food preparation where a lot of coriander leaves are used along with garlic, ginger and green chillies and are cooked with grated tomatoes and spices. This mixture is basically used as a base in many Sindhi preparations.
Another popular method of Sindhi cooking is Daas, where whole vegetables like apple gourds, bitter gourds or capsicum are stuffed with a mixture of grated onion and Sindhi pesto and cooked till tender.
Chef Satyajit Kotwal.
Chef Sanjeev Kapoor
1) What is the influence of other cuisines on Sindhi food?
Sindhi cuisine is a result of many influences. Since Balochistan touches the border of Sindh, and so does Punjab, there is bound to be an immigration of ideas. Pre-partition played a crucial role in shaping Sindhi cuisine. This cuisine also has some impact on the Mughals, Arabs, and Turks since all these dynasties ruled the Sindh province once. As Sindh was once part of India, Indian cuisine also has a significant influence on it.
2) What sets Sindhi cuisine apart from others? Is it their way of using vegetables, spices, or their way of cooking?
I feel it’s an amalgamation of both! They have a unique style of cooking and have their favourites when it comes to the addition of masalas. They like to play with the base of their dishes. Their most classic recipes either have a tomato or onion base or a ginger-garlicky with a heavy dose of spiciness. Yes! Sindhis like their food spicy. But, not all their food is fiery, there’s an array of sweets, snacks, and breads too in this wonderful cuisine to pick from. When it comes to vegetables, leafy greens like spinach (palak), fenugreek leaves (methi) & dill (savaa), and others like ladyfingers (bhindi), potatoes (aloo) & drumsticks (seeng) are extensively used. Apart from this, accompaniments are also imperative in a typical Sindhi meal. Dishes such as fried potatoes or fried bhindi, papads, dahi, sweet boondi, etc., are the most common ones.
3) What are the items that are your favourite?
My favourite food is Dal Pakwan but not forget their simple sabzi like bhindi bashar or the yummy sai bhaji… dishes like koki n lola feature on my breakfast menu some days. Another classic item that I love and will have soon during Holi is Gheeyar.
4) How is Sindhi Kadhi different from other Kadhis?
Sindhi Kadhi is so flavorful which is made using tomatoes and some besan but what I like the most is the veggies that go in it, gavar and bhindi. The element of dahi is missing in a Sindhi kadhi.
Three passionate agripreneurs from Hyderabad started SAGO Speciality Feeds in 2019 to build a fodder ecosystem among the dairy industry for feeding the dairy animals, thus driving increased milk yields. The production activity, they say, is directly beneficial and profitable to the farming community, dairy farmers, livestock and also the consumers.
New Delhi, March 26, 2021: Started in 2019, Hyderabad-based AgriTech startup — SAGO Speciality Feeds — is aiming to contribute to the dairy sector and the corn industry in India by making end-to-end mechanised corn-based silage with quality nutrients. By doing this, the company founded by three passionate agripreneurs, is promoting extensive cultivation of high-yielding biomass corn hybrids, suitable for livestock feed and sensitising the farming community to be a part of forage production – a high priority agricultural activity. The high-quality corn silage produced at SAGO’s Banswara, Rajasthan, plant helps build a fodder ecosystem among the dairy industry for feeding the dairy animals, thus driving increased milk yields.
In an exclusive conversation, one of its founders, Chandrasekhar Singh, takes us through his entrepreneurial journey in the Agri sector and talks at length about his passion project, its flagship brand of corn silage — CornvitaTM, and why giving cattle the right nutrition matters to him and his company. He says, “it is because this activity is directly beneficial and profitable to the farming community at large, the dairy farmers, the livestock and also the consumers at the end.” SAGO’s hardwork has been suitably rewarded — it is the only company in Rajasthan to make corn silage this season. Read on:
Q: Please take us through your entrepreneurial journey, from NABARD to Sago Feeds; how has it been so far?
Appearing for competitive examinations was a routine affair during my college days, and by the age of 22, I had three offers in government service to choose from, and I opted for NABARD, that too, before completing my graduation. It was a great pride for my parents as I joined the government service at a young age and in our hometown. Everything was smooth and happy, and in no time, I completed 29 years of service. I had the honour of serving NABARD for 27 years in Hyderabad and two years in Mumbai. Many-a-times, I felt like everything was moving in a formatted manner with not many challenges coming my way.
I always dreamt of being an entrepreneur, especially in the agricultural sector. It took almost four years of research and firming up the plan, and I finally decided to take the big leap. I quit my job at NABARD, and I was relieved on February 28, 2019; I registered my company on March 6, 2019.
Adding to my thoughts and strength was my nephew Saikiran, who was then working as a Quality Engineer in the US after completing his MS in Automobile Engineering. He quit his job and switched careers. We were joined by my son Anurag, who was working for Amazon. Today, three of us have come together from different professional backgrounds and skillsets from the same family to work on SAGO.
Founders of SAGO — (from left to right) Chandrasekhar, Saikiran and Anurag.
What is the story behind this name?
As we all three belong to the same family, we thought of launching a brand which is close to all of us. After all the brain-storming sessions, we finalised SA-GO, which is coined from the names of my mother (SA-thyavathi) and my father (GO-pal Singh). We launched our company SAGO Speciality Feeds (2019), and CORNVITA is our flagship brand of corn silage.
Why did you choose cattle feed? What research went behind choosing it? What is the market standing of cattle feed? Do people invest in buying good cattle feed?
Dairy was something that fascinated me, especially the feed sector. After a detailed study, I felt tremendous potential and dearth for dairy feed in India.
India has been the leading producer and consumer of dairy products since 1998, with sustained growth in the availability of milk and milk products. Dairy activities form an essential part of the rural Indian economy and serve as an important source of employment and income for the people.
India also has the largest bovine population in the world. However, per animal milk production is significantly low as compared to the other major dairy producers. Moreover, India’s dairy produce is consumed domestically, with the majority of it being sold as fluid milk. On account of this, the Indian dairy industry holds tremendous potential for value-addition and overall development. According to the latest IMARC Group report, titled “Dairy Industry in India 2021 Edition: Market Size, Growth, Prices, Segments, Cooperatives, Private Dairies, Procurement and Distribution”, the dairy market in India reached a value of INR 11,360 billion in 2020.
Poor nutrition and lack of proper feed management are the reasons for low milk yield. The non-availability of green fodder during summers and reliable production in monsoon are the biggest challenges today. Corn Silage is one such fodder supplements that address these challenges. Silage is not only delicious and more palatable for the cattle but also has the right amount of proteins, carbohydrates and acidity that ensures a healthier gut and improves overall health and fertility.
Silage is a fermented, high-moisture, stored green fodder fed to cattle, sheep and other ruminants; it can also be used as a biofuel feedstock for anaerobic digesters. It doesn’t contain any synthetic additives or chemicals. Silage also reduces the volume of feed as it is highly compressed, thereby decreasing the overall cost of feed and meeting the nutritional requirement. With its relatively high energy content, corn silage is also well adapted for low-cost rations for fattening cattle.
Silage is a fermented, high-moisture, stored green fodder fed to cattle, sheep and other ruminants. Silage can also be used as a biofuel feedstock for anaerobic digesters. It doesn’t contain any synthetic additives or chemicals.
CornvitaTM has an ideal balance of proteins, carbohydrates and several amino-acids. As silage is pre-digested food, cattle do not find it necessary to ruminate. As a result, ease of digestion increases, thereby improving the overall health of cattle’s gut. As proteins now can easily get digested and metabolised, the quantity of milk improves along with an increase in fat and SNF percentages.
We observed that most of the dairy entrepreneurs (small and big) lack the knowledge of the feeding system and guidance from experts. They lack the technical support and exposure to the best practices of feeding cattle. Most of the small farmers aim at the most economical way of feeding their animals without knowing the merits or demerits of the feed. But once they are enlightened with the results of using silage and balancing with other feeds, there is a tremendous shift in their approach and opt for silage.
What goes behind the scenes of producing silage, from start to finish?
The process of silage production is exciting and challenging. It needs meticulous planning and monitored at every stage. Growing maize crop for silage is highly beneficial for the cultivating farmers with higher yield and higher price per acre plus an additional season every year as the crop is harvested on the 80th day instead of 120 days.
We travelled extensively by road in Gujarat and Rajasthan to identify corn growing belts. Simultaneously, we also had a good number of meetings with large dairies with whom we could collaborate for sales. We could also meet a large group of farmers and FPOs from remote areas of Udaipur, Rajsamand, Chittorgarh, Bikaner, Barmer, Pratapgarh and Bhilwara districts.
Your plant is based in Rajasthan. Why did you choose Banswara?
Banswara district in Rajasthan is strategically located close to the border and close to three other states — Gujarat, Madhya Pradesh and Maharashtra. The rich soil and weather conditions are suitable for maize cultivation and added to this, the district is blessed with Mahi river with round the year water availability. Moreover, Gujarat and Rajasthan have the biggest dairies in India also have the largest cattle population. During our initial visits, we had to drive through hundreds of kilometres of maize fields. Also, it was easy to discuss with farmers who are already into maize cultivation.
How is the team at Sago Feeds structured? What is the supply chain like; please explain?
SAGO Speciality Feeds has bloomed from within a single-family. We all share responsibilities depending on our skill sets. I take care of the operations, management and planning.
My nephew Saikiran has experience in manufacturing and supply chain. He drives overall strategic vision and direction.
My son Anurag heads product development and marketing. He holds the experience of leading several life-science research projects, digital marketing and has worked for Amazon in the last mile analytics and quality team.
Silage production is directly beneficial and profitable to the farming community at large, the dairy farmers, the livestock and also the consumers at the end.
Who are the primary beneficiaries? How do you market and sell your products? How has been the response so far?
Our activity is something that is directly beneficial and profitable to the farming community at large, the dairy farmers, the livestock and also the consumers at the end.
Marketing and sales are challenging at the beginning. It is difficult to reach the dairy farmers and convince them about the benefits of silage. We usually give them a demonstration of our product and sometimes give them samples to use. Even humans have a reluctance to anything new, and the same is the case with animals. But once they are used to this feed, it is a cyclic action, and there is always continuous demand. Seeing is always believing, and when the farmers witness the results for themselves with higher milk production within 6-8 days and higher Fat & SNF percentage, they tend to shift to this feed.
Currently, we have committed demands from Banas Dairy, Gujarat, and Parag Dairy, Maharashtra, Miraj and Bhilwara Dairy, Rajasthan and many others around our location. We have continuous supplies to Palanpur, Mehsana, Anand, in Gujarat, Rajsamand, Udaipur, Pratapgarh in Rajasthan and Indore, Bhopal, Dewas in Madhya Pradesh, Nasik and Ahmednagar in Maharashtra. We have also started supplies to places as far as Chhattisgarh and Telangana. We keep getting enquiries from places like Karnataka and North East. This itself shows the huge demand and also dearth of the product.
Incidentally, we are the only company that made corn silage this season in Rajasthan. The response is so huge that we have nearly 10,000 MT of demand on hand, but we have only 3,100 MT of material to supply.
We travelled extensively at regular intervals within Gujarat and Rajasthan, including the border districts like Bikaner in Rajasthan and Kutch in Gujarat. Farmers are excited to use the product, which is beneficial for them. After all our meetings across the states, we felt most of the farmers are still ignorant of the latest developments, technology, science and are not aware of the best practices of feeding their animals. Incidentally, Banas Dairy, Gujarat, is collaborating with us to train and sensitise the farmers on the use and making of silage in Gujarat.
What were the major challenges in your entrepreneurial journey? How did you overcome them?
Switching my career — from being a Government servant to becoming an entrepreneur — was a 360⁰ shift in my thought process. I could really experience the transition of this journey and I can say these two are poles apart from one another. Earning money was not my prime goal but building a system that is consistent and sustainable was. Meeting farmers from across the states and being one among them was always an enriching experience. Our success can only be measured with our reach, growth and prosperity of the farmers.
Reaching farmers and sensitising them about our activity was a difficult task. Not everyone is inclined towards this shift in the cultivation of corn crop and a shift from the age-old feeding system to their cattle. Initially, we started our supplies at a few of the big dairies, their feedback made all the difference and that made a beginning in our supplies.
Who are the other players in this market?
Punjab and Haryana are the leaders in India’s silage production, with nearly 1.5 lakh MT of production every year. There are 4-5 big companies all based in Punjab, which cater to most states’ needs. There are 3-4 other companies scattered in Karnataka, Maharashtra and Madhya Pradesh, which are into silage production.
What are your plans for SAGO?
After completing three production cycles in three different states, we now plan to replicate the process in different places to cater to a particular zone, cutting down the transportation costs. We plan to set up small pockets/points wherein we can stock the material for supplies to the nearby places. We hope to start our activities closer to Odisha/Chhattishgarh for the eastern states, Indore/Bhopal for the central parts and then continue at Rajasthan to cater to the needs of Gujarat and Maharashtra.
Silage conventionally is seen as a premium feed by dairy farmers. The present challenge of handling and wastage of the product makes the purchase feasible only for large dairy farmers to purchase. We are re-working our strategies and challenging the status quo to make our product available to every dairy farmer across the country. Not just that, we also have plans to start a few initiations in the food sector soon.
(Text by Shillpi A Singh and images sourced from SAGO)
The one-of-its-kind service by Practo will provide 24*7 remote consultations by licensed veterinarians for pets healthcare needs.
New Delhi, March 24, 2021: In a bid to create equitable healthcare access for all, Practo, India’s leading integrated healthcare company has launched veterinary telemedicine service on its platform. Teaming with licensed veterinarians across the country, the company will be offering 24*7 online consultation services for pets.
Launched as a pilot project last month, Practo recorded nearly two lakh search queries from pet parents. Buoyed by the positive response, the speciality was launched officially as a part of the company’s telemedicine services. Most of the veterinary queries revolved around diet management for pets, medication for fleas and ticks, food allergies among pets, and behavioral problems among pets. Queries came in from more than 40 cities with Bengaluru, Hyderabad, Delhi NCR, and Mumbai topping the list.
Commenting on the new initiative, Siddhartha Nihalani, VP – Product, Practo, said, “Our foray into virtual veterinary care aligns with our larger vision of improving access to quality healthcare. With many people taking care of pets for the first time during the Coronavirus-induced lockdown, and several others anxious about visiting a clinic amid this pandemic, we want to enable them with a convenient yet reliable solution.”
Online veterinary consultations become even more convenient once the work from home situation ends, as pet parents can consult online whenever they have concerns without skipping work. This includes getting a second opinion for certain procedures, obtaining treatment or diet recommendations, asking follow-up questions, and seeking advice on behavioural issues – all in real-time and without exposing themselves to any risk.
Dr Daisy Rani, a veterinarian from Chennai with 25 years of experience, said, “Helping people to take care of their pets is the best part of being a veterinarian. Being able to do that in a way that is convenient for pet parents, especially during a pandemic like this, is a truly rewarding experience. I am glad that a company like Practo is going the extra mile for the well-being of pets by adding veterinary services as a part of its telemedicine platform.”
With Practo’s veterinary telemedicine service, pet parents can connect with a verified veterinarian via audio or video call or even text messages – anytime, anywhere – in just 60 seconds. Not only is this convenient, but also crucial to get timely advice on common but potentially harmful ailments. The service will be available both on Practo’s app as well as the website. To consult a veterinary doctor online, click here.
World TB Day 2021: Tuberculosis kills more number of people in India every year than the lives COVID19 has claimed over the past 12 months? Today, all we need is a surge in our actions to reduce the TB burden, tells Dr Anshu Punjabi.
New Delhi, March 24, 2021: In the past year, the COVID19 virus grabbed much of our attention. The collateral damage that it caused in one year is very unimaginable. But did you know, Tuberculosis (TB) kills a more significant number of people in India every year than the lives COVID19 has claimed over the past 12months?
Tuberculosis continues to inflict a large quantum of socioeconomic cost on our nation. Although TB has been curable and our government has made great strides to improve diagnosis and drug delivery mechanisms, our war with this deadly disease exists. All we need today is a surge in our actions to reduce the TB burden intensely. But how is that possible?
Well, the best approach to this is to sensitize people with the growing burden of TB and empower them enough to identify symptoms, report it early, undergo timely diagnosis, and complete adherence to treatment. So, first things first.
WHAT IS TUBERCULOSIS AND HOW DOES IT AFFECT US? TB is an infection caused by bacteria called Mycobacterium Tuberculosis and spreads through the air from one person to another when an infected person coughs, sneezes or laughs. Even though the bacteria travel easily, it’s not easy to be infected by TB. Most often, it’s spread between family members, close friends, and people who live or work together. TB most commonly affects the lungs, but it can affect other parts of the body as well, like lymph glands, abdomen, spine, joints, etc.
There are two kinds of tuberculosis (TB) infections — latent TB and active TB disease.
WHAT IS LATENT TB? In most healthy people, the body’s natural immune system kills the bacteria and there are no symptoms. Sometimes, the immune system cannot kill the bacteria but manages to prevent it from spreading in the body. You will not have any symptoms, but the bacteria will remain in your body – this is known as Latent TB. People with Latent TB are not infectious to others, and do not feel ill. It is usually happens to children. Sometimes, this dormant TB gets activated when the body’s immune system is extremely low, say in the case of HIV, cancer, diabetes, etc.
This may occur like a normal fever and can go unnoticed. In India, we do not treat latent TB, as most people would have been exposed to the bacteria at some point in time. Moreover, there is no good evidence that all these people will develop active TB disease in the future, or that treating Latent TB will prevent further reinfection.
WHAT IS AN ACTIVE TB? When the immune system is unable to kill or contain the bacteria, Active TB develops. The lungs’ Active TB disease is contagious, which means it can be spread from one person to another. It is most often spread through the air; these bacteria may enter the air when a person with TB disease of the Lungs or throat coughs. People nearby may breathe in these bacteria and get infected. People get sick from the TB bacteria that are alive and active.
SO, WHAT ARE THE RISK FACTORS?
Being in close contact with a person with Active Lung TB disease is highly risky
If you are in contact with any groups known for passing on TB, such as the homeless, injection drug users, and persons with HIV/AIDS
If you are living or working with people who are at high risk for TB, such as those in hospitals, homeless shelters, prisons, slums, or refugee camps
MAJOR SIGNS AND SYMPTOMS THAT YOU SHOULDN’T IGNORE:
A cough that lasts two-three weeks or more
Pain in the chest, with cough or at rest
Coughing up blood or thick mucous
Night sweats
Feeling weak or tired
Weight loss
Not wanting to eat
Fever, mainly in the evening
Swollen neck lymph-gland(s)
The longer people wait, the TB disease worsens. Although the stigma associated with TB has gone down significantly, people need to be alert, aware, and responsible when it comes to identifying symptoms and getting treated early. TB is treatable and curable. Treatment for drug-sensitive TB is a combination of antibiotics for six months. People with drug-resistant TB will need more extended treatment with at least 5-6 drugs under expert supervision.
(Dr Anshu Punjabi is Consultant-Pulmonologist & Sleep Medicine Expert, Fortis Hospital, Mulund; Image by Wilfried Pohnke from Pixabay)
Women are redefining the age to be a mother, and thanks to advancements in technology surrounding fertility, pregnancy, and delivery, it’s possible to have a baby after 40.
On World Water Day, Dr Sonali Gautam explains poor water hygiene’s impact on one’s health, especially children.
New Delhi, March 22, 2021: On World Water Day, while we all should aim to save the most precious gift and a vital life source, we must also focus on improving water supplies and hygiene. You must be wondering why, so let me explain the impact of poor water hygiene on health. Worldwide, 2.2 billion people lack access to safely managed drinking water, and 4.2 billion people lack safe sanitation. Unsafe hygiene practices are widespread, compounding the effects on people’s health. The impact on child mortality rates is devastating, with more than 2,97,000 children under five die annually from diarrhoeal diseases due to poor sanitation, poor hygiene, or unsafe drinking water.
In India, the problem of unsafe water is a substantial public health concern. Apart from illnesses such as diarrohea, jaundice, etc., unsafe water also contributes to Hepatitis A & E. Both these diseases are associated with inadequate and unsafe water supplies, poor sanitation & hygiene, leading to infection and inflammation of the liver.
What is Hepatitis A and E? Hepatitis A and E viruses are RNA virus, which primarily infects the liver, causing inflammation of the liver (Acute Hepatitis). Infection with Hepatitis A & E is usually self-limiting.
How is the infection acquired? Hepatitis A or E is spread primarily through food or water contaminated by faeces from an infected person (feco-oral route). It enters the liver from our gut and is then excreted again by our gut into the stool, thus completing the infection cycle.
Who are at risk for Hepatitis A or E? Not everyone who’s infected will have any evidence of this disease, as it may go unnoticed (asymptomatic disease). But still, these people can excrete viruses in their stool and continue to infect others (carriers).
Asymptomatic disease: India being a developing nation with poor sanitation conditions, more than 95% of children below five years of age are usually infected with these viruses, with an asymptomatic course. Thus, in India, antibody to Hepatitis A virus is nearly universally detectable by adolescence, and antibody to HEV increases during young adulthood to reach about 40% in adults.
How does it spread? Hepatitis A is usually spread person-to-person through food or water contamination. An infected person’s hands can become the source of infection after using the bathroom. The virus then spreads by direct contact or by food, beverages or other objects that the infected person handled. An infected individual can transmit the virus to others as early as two weeks before the symptoms begin to appear.
Symptomatic disease: International travellers to India, children from high-income families are at risk of developing Hepatitis A or E infection because they do not eat much from the streets and have not developed the required antibodies resulting in fever, stomach-ache and jaundice.
What are the symptoms of Hepatitis A or E?
Fever
Tiredness
Stomach upset
Loss of appetite
Dark yellow urine
Diarrhoea
Yellowish eye & skin called jaundice
Why is it dangerous? Unlike Hepatitis B & C, Hepatitis A does not cause Chronic Liver Disease and is rarely fatal. But it can cause debilitating symptoms and Fulminant Hepatitis (Acute Liver Failure), which is often fatal. Fulminant Hepatic Failure leading to death is seen in 1.8 % adults, and 10% in pregnant ladies.
Most people with Hepatitis E get better within a few months. Usually, it doesn’t lead to long-term illness, or Liver damage like other forms of Hepatitis do. But Hepatitis E can be dangerous for pregnant women or anyone with weak immune systems, including the elderly or ill.
How to prevent it? The best approach is to take all precautions to avoid Hepatitis and ensure safe drinking water for all. Make sure that your water source is clean and well maintained. Apart from this, follow this:
Hand sanitation: Frequent handwashes before meals and after using the washroom.
Avoid eating outside, especially if you are pregnant.
Hepatitis A vaccine: Vaccinate your children below six years (consult a paediatrician about this).
If you identify any of the above symptoms, kindly meet your Gastroenterologist for timely treatment and care to resolve the infection with expected full recovery.
(Dr Sonali Gautam, Consultant-Gastroenterology, Hiranandani Hospital, Vashi, a Fortis network hospital; Image from Pixabay)
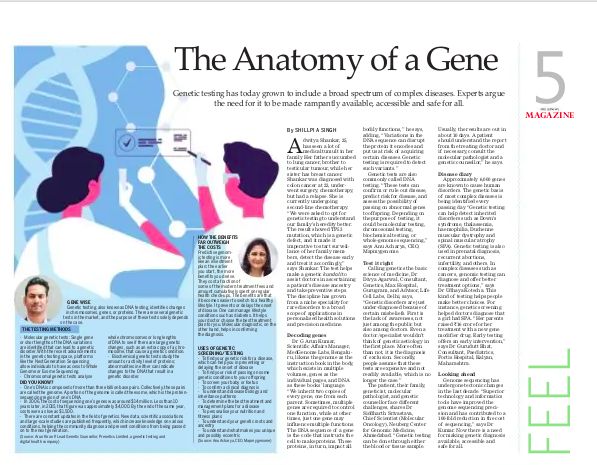
Genetic testing has grown from a niche speciality for rare disorders to a broad scope of applications for routine, complex diseases to its use in personalised health solutions and precision medicine. There is a need for healthcare providers, the diagnostic community and the government to step-up and uplift genetic diagnostics, making it available, accessible and safe for all.
Dr G. Arun Kumar, Scientific Affairs Manager, MedGenome Labs
Dr G. Arun Kumar, Scientific Affairs Manager, MedGenome Labs.
Explain genetic testing/screening to a layman. What are the challenges of genetic testing?
To understand genetic testing, it is essential to understand the role of DNA and genes in our bodies. We can see our genome as the instruction book in our body which exists in multiple volumes, the genes as the individual pages present in these books, while the DNA is the language in which the pages are written. Genes regulate specific parts or functions of a cell. We inherit two copies of every gene, one from each parent. Sometimes multiple genes are required to control one function. Other times, just one gene may influence multiple functions. The DNA sequence of a gene is the code that instructs the cell to make proteins. These proteins, in turn, affect all bodily functions. Any variations in the DNA sequence can disrupt the protein it encodes and put us at greater risk of acquiring certain diseases in our lives. Genetic testing is a tool used to look at our DNA to detect such variants. Results from a genetic test can significantly help doctors understand the cause of a disease or symptoms, predict an individual’s risk of developing certain diseases, tell if one could pass the disease to their children and help in choosing the best treatment that can be tailored for the individual. For instance, if a person has cancer, then a genetic test can tell if the person inherited a cancer-causing genetic aberration. Early detection can also help doctors make an informed decision about the same and tell if the patient is at risk of developing any other type of cancers as well. Genetic testing of cancer tissue can help in identifying genetic variants that can be targeted using specific drugs.
Performing genetic testing requires high expertise both in terms of laboratory testing and analysis of genetic data. Understanding a genetic testing report for a commoner requires a clinician or a genetic counsellor.
If I have hereditary spherocytosis, can I get to know the chances of it being carried by my offspring and how?
In most cases, spherocytosis occurs as an inherited disease that changes and reduces the life of red blood cells in the patient’s body and causes anaemia. The initial evaluation of hereditary Spherocytosis involves a physical inspection, a review of the family history, and few lab tests on blood samples. In Spherocytosis, the structure of red blood cell changes, attributable to a defective protein produced in the cell due to genetic mutations. Genetic testing for spherocytosis looks for variants in the genes ANK1, EPB42, SLC4A1, SPTA1, SPTB. Some of these genetic variants are inherited in an “Autosomal recessive” manner. It means that for a person to express the disease (s)he must inherit genetic variants in both the gene’s copies. If a person has inherited a genetic variant in only one copy of the gene, the other copy being healthy, then this person is termed as a carrier. A person with the disease will 100% pass on one defective copy of the gene to the offspring. On the other hand, an individual who is a carrier has a 50% chance of passing the offspring’s variant. In either case, if the partner of the individual also passes on one defective copy to the offspring, then the child will develop the disease.
What are the things to keep in mind while opting for genetic testing/screening? What are its hope for medical science in the days to come?
Genetic testing can help in identifying an inherited disease risk in an individual. It is important to discuss the reasons for a genetic test with your doctor as they may guide you to a medical geneticist who is trained to diagnose a genetic condition, select the appropriate genetic tests, explain the test results, and recommend personalized treatment and prevention options. Before opting for genetic testing, one should gather as much information as possible about the family’s medical history to understand the risk better.
What are the diseases for which this screening works?
MedGenome currently offers more than 475 genetic tests across several disease categories such as paediatrics, neurology, oncology, haematology, endocrinology, nephrology, ophthalmology, etc. Any disorder that has an established genetic basis can be screened. Additionally, we also offer carrier screening for couples that will tell the carrier status of various genetic variants in the couple. This shall aid the clinician counsel the couple for future pregnancy.
What are the services offered by MedGenome?
Medgenome offers genetic testing services under four major divisions, viz – Actia, Claria, Prima and Micra. The Actia division deals with genetic testing of all inherited disorders encompassing all major medicine disciplines, including neurology, ophthalmology, cardio-vascular, Metabolic disorder, Nephrology, etc. The Claria division deals with reproductive genetics that offers various prenatal genetic testing panels, NIPT, and pre-implementation genetic testing. The Prima division deals with Oncology (solid tumours and Leukaemia) and Hematology range of testing. All these tests are College of American Pathology accredited. The Micra division is a new addition to our portfolio that is involved in infectious disease testing. In this range, we have indigenously developed the first whole genome sequencing of Mycobacterium tuberculosis directly from a patient’s sputum.
MedGenome is the market leader in India’s genetic diagnostics and is one of the largest high- throughput NGS sequencing labs in South Asia. We possess state-of-the-art Next-generation Sequencing (NGS) facility, which houses cutting-edge genome sequencing platforms such as Illumina’s NovaSeq, HiSeq X, HiSeq 4000 and 2500, MiSeq, etc. A sophisticated IHC pathology lab supports our Sequencing facility. We also offer other genomic testing technologies such as FISH, PCR, Sanger Sequencing, and Microarray to offer comprehensive diagnostic solutions to clinicians, hospitals and researchers. We offer genetic testing at different scales such as identification of point mutations using Sanger technique, RT-PCR; chromosomal level aberrations using FISH, Chromosomal microarray; multigene and whole-genome sequencing using Next Generation Sequencing
Is genetic testing gaining popularity?
Genetic testing is gaining popularity among all medicine disciplines because of its wide applications inpatient management and family planning. Almost all significant guidelines of different medical disciplines have incorporated genetic testing in their statements. The awareness of genetic testing among the general public is also increasing so much so that direct consumer testing for personal genomics is not far from reality.
What are the cost implications?
Genome sequencing technology has undergone tectonic changes in the last decade. The development of superior technology and informatics tools has improved genome sequencing precision and has contributed to a 100-fold reduction in sequencing cost. MedGenome has been a forerunner in India for democratising genome sequencing by making it affordable, beyond the reach of a commoner a decade ago, without compromising the quality.
Arun Kiran P, Lead Genetic Counsellor, Prenetics Limited
Arun Kiran P, Lead Genetic Counsellor, Prenetics Limited.
Explain genetic testing?
Genetic testing, also known as DNA testing, is a process of identifying changes in chromosomes, genes, or proteins.
Genetic testing results can help individuals either confirm or rule out the possibility of having a clinical condition; identifying genetic mutations can determine a person’s chance of developing genetic predisposition risk or passing on a genetic disorder.
There are several genetic tests in the market, and the purpose of these tests solely depends on the case and the scenario it is in use. Several methods are used for genetic testing:
Molecular genetic tests: where single genes or short lengths of the DNA variations are identified that can lead to a genetic disorder. With the recent advancements in the genetic testing space, platforms like the Next Generation Sequencing allow individuals to access Whole Genome or Exome Sequencing (WES).
One’s DNA is composed of more than 3 billion base pairs. Collectively, these pairs are called the genome. A portion of the genome is called the exome, the protein-sequencing region of one’s DNA.
Chromosomal genetic tests analyse whole chromosomes or long lengths of DNA to see if there are large genetic changes, such as an extra copy of a chromosome, that cause a genetic condition.
Biochemical genetic tests study the amount or activity level of proteins; abnormalities in either can indicate changes to the DNA that result in a genetic disorder.
2) If I have hereditary spherocytosis, can I get to know the chances of it being carried by my offspring and how?
Hereditary spherocytosis is a condition characterized by haemolytic anaemia (when red blood cells are destroyed earlier than normal).
Signs and symptoms can range from mild to severe and may include anaemia, pale skin, fatigue, jaundice, gallstones, and/or enlargement of the spleen. Severe cases involve short stature, delayed puberty and skeletal abnormalities.
Mutations cause this condition in any of the several genes, such as the ANK1, EPB42, SLC4A1, SPTA1, and SPTB genes. It is most commonly inherited in an autosomal dominant manner but may be inherited in an autosomal recessive manner in rare cases. Different types of hereditary spherocytosis are distinguished by severity and genetic cause.
Autosomal Dominant Inheritance:
About 75% of cases of hereditary spherocytosis are inherited in an autosomal dominant manner. This means that having a change (mutation) in only one copy of the responsible gene in each cell is enough to cause the condition.
When a person with a mutation passes on to the child for an autosomal dominant condition, each child has a 50% (1 in 2) chance to inherit that mutation.
In rare cases, hereditary spherocytosis is inherited in an autosomal recessive manner.
A person must have inherited one mutated gene copy from each parent, who are referred to as genetic carriers.
When 2 carriers of an autosomal recessive condition have children, each child has a:
– 25% (1 in 4) chance to be affected
– 50% (1 in 2) chance to be an unaffected carrier like each parent
– 25% chance to be unaffected and not be a carrier
Carriers of an autosomal recessive condition typically do not have any signs or symptoms (they are unaffected). By doing a full gene analysis of these genes, one can understand the risk of passing it on to their offspring.
Any interesting case study or success story?
Ms Roopa, who is in her early 30s from Bangalore, reached out to me as she had a strong family history of breast cancer on the maternal side of the family. Ms Roopa’s mother and maternal aunt were diagnosed with breast cancer in their 40s and she was very worried about her potential risk of being diagnosed with Breast Cancer in future. As a genetic counsellor, I explained to Ms Roopa about the potential chances of inheriting a genetic mutation in one of the cancer-causing genes associated with breast cancer based on the family history she had described.
Ms Roopa was suggested to get her mother tested for a hereditary cancer panel consisting of breast cancer-causing genes. Based on the hereditary breast cancer panel analysis, it was found that Ms Roopa’s mother had a genetic mutation in PALB2 gene, which is strongly associated with Breast cancer, and this mutation is also known to increase the risk of pancreatic cancer and ovarian cancer.
The genetic mutation that was detected in Ms Roopa’s mother was tested for Ms Roopa and based on the analysis the same genetic mutation was inherited in the PALB2 gene. This led to an understanding that Ms Roopa has an increased risk for the above-mentioned hereditary cancer conditions.
As the genetic mutation present in the gene PALB2 follows an autosomal dominant mode of inheritance where there is 50% chance for the genetic mutation to be passed on to the offspring. Based on these interpretations and findings, specific screening and surveillance measures were suggested to Ms Roopa based on the National Comprehensive Cancer Network® (NCCN®). Due to the genetic mutation being present the surveillance and screening needs to start as early as the age of 30 onwards considering the family history and clinical data.
Ms Roopa was suggested to do Annual mammography with consideration of tomosynthesis along with consideration of annual breast MRI with contrast starting at age 30, with modification as appropriate based on family history by discussing with the physician.
Potential management options such as prophylactic risk-reducing mastectomy (surgery to remove one or both breasts to reduce the risk of developing breast cancer by up to 95%) was suggested as an option by having a discussion with the oncologist based on the family history.
Knowing if a PALB2 genetic mutation is present is advantageous. At-risk relatives, i.e., first/second-degree relatives, can be identified, enabling the pursuit of a diagnostic evaluation.
Getting the genetic test done has helped Ms Roopa be more proactive about her health and do these screenings from an early age onwards to help in potentially detecting any breast cancer tumours at the early stage of cancer for better treatment management purposes as most of the cancers do not show immediate symptoms and go undiagnosed till late stage of cancer-causing lesser chances of survival.
As a genetic counsellor, all the questions related to risk assessment, limitations of the genetic test, screening and surveillance options, and management options were discussed with Ms Roopa by giving her access to the right set of resources and a specialised doctor who can help her with overall process. More insights were provided based on the genetic findings to Ms Roopa and she was able to take her own choice based on the options provided by the genetic counsellor and the physician.
What are the things to keep in mind while opting for genetic testing/screening? What is its hope for medical science in the days to come?
Every genetic test is performed based on the situation. Individuals need to talk with their physician, geneticist or genetic counsellor to have a better understanding, especially when it comes to a diagnosis or a clinical condition.
There are things to keep in mind before deciding on a genetic test. Such as the test platform, test limitations, laboratory accreditations, measures taken to safeguard data and privacy, ability to access raw data. And most importantly, having access to genetic counsellors to understand the results to avoid undue stress and misinterpretation.
Accessibility of genetic tests has been dramatically increasing, and prices are still dropping to this day.
In 2006, the cost of sequencing one’s genes dropped to around $14 million. Less than ten years later, in 2015, that figure dropped to approximately $4,000. By the end of the same year, costs were as low as $1,500.
There are constant updates in the field of genetics. This means new data, scientific associations and massive large-scale studies are published frequently, which increases knowledge on various conditions. This indeed helps the community diagnose and prevent conditions from being passed on to the next generation.
Due to an increase in budget for research and development in the field of medical sciences, drug discovery and gene-therapies will be available for many rare conditions. This includes common health conditions that leads to personalised health solutions and precision medicine.
What are the services offered by Prenetics Ltd and what are the cost implications?
Depending on which CircleDNA kit one chooses, we provide different sets of information.
Vital kit (HK$1,192 ~ 11k INR) includes reports across 14 categories centring on diet, nutrition, fitness and overall wellness
Health kit (HK$3,192 ~ 30k INR) includes reports in four categories looking at health risks such as cancer and disease
Family Planning kit (HK$3,192 ~ 30k INR), made for those planning to conceive, is focused on the assessment of your carrier status for hereditary conditions.
Premium kit (HK3,992 ~ 37k INR) is the most comprehensive genetic test in the market, which offers more than 500+ reports across all categories.
Note that the CircleDNA results are not medical advice or report. They should not be used for diagnostic purposes. These tests are strictly meant to help individuals understand their genetic predispositions, where the results can be used to personalise their recommendations for optimum health.
What are the numbers like? Is it popular or gaining popularity?
The CircleDNA direct-to-consumer test under Prenetics Ltd has been quite popular in Asia, South East Asia, UK and in European countries.
On an average the lab processes more than 15,000 samples per month.
What is the turnaround time for the test?
From the sample collection to the test results being ready in the CircleDNA app, the process takes around 3-4 weeks of time. The testing process is very simple. Using a cheek swab in the DNA collection kit, collect a saliva sample and send your sample back to the lab.
What are the diseases for which this screening works?
CircleDNA is a comprehensive genetic test which consists of 500+ reports and tests for categories like Diet and Nutrition, Well-Being, Stress and Sleep, Pollution, Skin, Talents and Sports, Sports and Fitness, Success Traits, Music and Dance, Ancestry Test Results (with up to 15 geographical categories), Personality Traits, Behavioural Traits, Physical Traits, Gender Traits, Carrier Screening for understanding the risk of passing on the risk to the child (Family Planning), Hereditary Cancer risk.
The test helps an individual understand if h/she has inherited any mutation, increasing the risk for Cancers with a genetic basis, Dementia & Brain Health, common health risks such as obesity, stroke, and type 2 diabetes. Such health risks are very prevalent among the South Asian population.
Dr Gurudutt Bhat, Consultant – Paediatrics, Fortis Hospital, Kalyan
Dr Gurudutt Bhat, Consultant – Paediatrics, Fortis Hospital, Kalyan.
What are the opportunities and challenges of genetic testing?
The COVID19 pandemic has truly showcased India’s medical engineering talent, scientific expertise and the country’s potential to become a healthcare hub of the future. In this growth story, what stands out is India’s vast opportunity to achieve dramatic improvements in health outcomes. One way to that is genetic testing. Genetic testing has come a long way in preventive medicine, especially among pregnant women and their babies.
Blood and other tests are done mainly in pregnant women to rule out any diseases caused by a defect in the baby’s genes. It helps the expectant mother and her treating Obstetrician to manage the pregnancy and delivery appropriately. Some of the defects which can be detected are of the baby’s brain or spine etc. It can be an invasive test like a blood test or Amniotic Fluid Test, or non-invasive test like Ultrasonography. After the baby is born, its genetic sequencing can help confirm any gene mutations’ presence or absence. If the family already has an older child with genetic disorders, this test will help the subsequent baby be diagnosed early, and appropriate intervention can be initiated.
A great example of genetic screening is in older women who get pregnant after the age of 34yrs. These women are at high risk of having babies with Down’s Syndrome. Since it is a genetic disorder, the early screening will help detect such defects. This allows the family understand the consequences of the defect. They can undergo appropriate counseling, and it also helps the mother deliver the baby with proper precautions.
The biggest challenge for the success of genetic testing in India is its high cost. However, with the increasing use of genetic screening in India, the cost factor is slowly balancing out. Another problem area is that like everything else in medicine, this is not an exact science. There is a lot of evidence that still needs to be organized. There may be some problems with the tests available with some genetic testing companies, and not all tests are available easily in India.
When does genetic disorder get transmitted from a mother to her baby?
The defects in a mother’s X chromosome can be inherited by both male and female babies. A defect in Y chromosome can only be detected in a male baby. A defect in the other chromosome can be transmitted to a baby in two forms known as autosomal dominant i.e. the gene will express dominantly in the baby even if there is only one copy of that gene on a chromosome. In an autosomal recessive genetic conditions both copies of the gene are needed for expression.
If I have hereditary spherocytosis, can I get to know its chances being carried by my daughter?
Hereditary spherocytosis is a genetic defect leading to a defect in the spectrin protein, which make the red blood cell membranes fragile. This red blood cell breakdown causes anemia and its complications. Up to 75 % of hereditary spherocytosis cases are autosomal dominant gene induced hence can be seen in babies of mothers with this condition. Hence, early diagnosis and proper treatment can prevent complications.
Any interesting case study or success story?
A recent case of a girl with the genetic problem of Spino-Muscular Atrophy can be a classic example of a success story. Due to genetic screening, doctors were able to diagnose her medical condition. Her parents raised Rs 16 crores for her treatment with a new gene modifier drug. This is a testimonial to the future where early genetic testing can help find a cure and offer early interventions for some genetic conditions.
What are the things to keep in mind while opting for genetic testing?
The idea for seeking genetic testing is to find way to prevent or treat certain conditions that we might be predisposed to. Decide which screening tests you need (to find a disease at an early stage when it might be more treatable), is important, so seek advice before testing:
Think about your reasons for wanting the test
Get the right tests
Ensure that you and your family are prepared for the results
Ensure that you have a personalized plan for dealing with the diagnosis
What is its hope for medical science in the days to come?
Genetic testing can help people make healthy choices. For instance, in a family that is predisposed to developing a certain kind of Colon Cancer or any other factors that can cause Cancer, genetic screening can help identify this risk. The opportunities this discipline offers for arriving at better health outcomes and personalized medicine are immense. We must realize that genetic testing has grown from a niche speciality for rare disorders to a broad scope of applications for routine, complex diseases and personal use. However, there is a need for healthcare providers, the diagnostic community and the government to step-up and uplift genetic diagnostics, making it available, accessible and safe for all.
Dr Udhaya Kotecha, Lead Clinical Geneticist, Neuberg Centre of Genomic Medicine
Dr Udhaya Kotecha, Lead Clinical Geneticist, Neuberg Centre of Genomic Medicine.
If I have hereditary spherocytosis, can I get to know its chances of being carried by my daughter?
Hereditary spherocytosis is a condition where hemolytic anemia occurs due to destruction of red blood cells. Currently, five genes are known to be causative for this disorder (genetic heterogeneity: where a single disease can be caused by genetic disease, causing variation in more than one gene). A patient suspected of having hereditary spherocytosis can have the same due to genetic variation in any one of the five genes. It is commonly inherited in an autosomal dominant manner, meaning that if one of your gene copies is carrying the variant, you may manifest symptoms. There is a 50% chance that each of your offspring may inherit the disease-causing variant in this inheritance pattern. Rarely hereditary spherocytosis is caused by recessive mutations: meaning that both copies of the gene need to be alerted to have the disease. If you have hereditary spherocytosis due to a recessive mutation, the chances that your children will be affected depends on your partner’s carrier status. If your partner is also carrier, a disease-causing variant in the same gene, then there is a 75% chance of your children being affected. If your partner does not carry any genetic alteration in the same gene, then all your children will only be carriers, but none will be affected.
Dr Siddharth Srivastava, Chief Scientist (Molecular Oncology), Neuberg Center for Genomic Medicine
Dr Siddharth Srivastava, Chief Scientist (Molecular Oncology), Neuberg Center for Genomic Medicine.
What are the challenges of genetic testing?
The patient, their family members, consulting clinician/ medical geneticist, molecular pathologist, and genetic counsellor have stakes in the successful resolution of the patient’s problem. Interestingly all of them face different sets of challenges. Finding the genetic basis of diseases is a matter of speciality doctors. The first challenge the patient faces is navigating their way from general practice to these centres that are usually located in cities or large towns. The rarefied set of specialists doctors are further split into sub-speciality. Doctors who understand genetic basis of cancers or that of cardiovascular disorders, inherited diseases etc. To get to the right doctor, often naïve patients have to go through a maze of trial and error.
A conclusive diagnosis of such disorders or disease can be made by using molecular techniques. A dialogue between the consulting doctor and molecular pathologist sets up where the molecular pathologist understands the patient’s clinical history and clinician’s question. Accordingly s/he selects right test using most appropriate technique. This is crucial as molecular tests are complex, running into weeks and they are also expensive. For most accurate reports, the molecular pathologist should get detailed and accurate patient history which helps them to correlate molecular data and write accurate interpretations which will have deep implications on patient management. Acquiring patient’s clinical history is a challenge.
A lot of the times, diagnosis of the patient has implications on the immediate family members such as children, siblings, children of siblings. During the time of diagnosis of the patient, the “at risk” family members may seem to be leading a normal life. They do not feel concerned about their own chances of getting the disease in later parts of their lives. Genetic counsellors face tremendous challenges by collecting data from various family members and discussing the risks and convincing them to take the test.
Any interesting case study or success story?
Genomic testing has made both detection of inherited disorders, as well as treatment of complex diseases such as cancer and there, are countless success stories. There was a person from Mumbai whose mother (70 years old) was detected with breast cancer (ER+Her2- type). An extremely sharp cancer doctor was treating her with hormone therapy. After three years of treatment, she relapsed. This means that she stopped responding to the hormone treatment and the tumour grew despite getting the therapy. The doctor discussed with us at Neuberg Center of Genomic Medicine, and based on the clinical history, we predicted that most likely a defect in either ESR1 gene or PIK3CA gene may have resulted in the patient no longer responding to the treatment. If the defect was indeed in ESR1 gene, the doctor could changer her therapy to a drug called fulvestrant, and if the defect were in PIK3CA gene, then the drug would have changed to Alpelisib (approved by US FDA). However, the problem got compounded as the patient moved out of Mumbai, and the amount of tumour tissue was less to perform the test. We resorted to another test call liquid biopsy, where a tube full of patient blood was collected from her home and shipped to our laboratory. Indeed we detected a defect in PIK3CA, and the patient is now doing very well on Alpelisib therapy.
Another instance was that of a 45 years old man from Nashik who had prostate cancer. Since he was diagnosed at a young age with cancer, the clinical doctor suspected it to run in the family. The doctor connected with us, and one of our genetic counsellor spoke with the patient at length to get a history of cancers in the extended family. Patient’s mother had breast cancer at the age of 55, and she had since passed away. Genetic counsellor converts entire patient’s family history into the pedigree chart. Defects in BRCA genes and BRCAness genes could be the reason for the patient’s prostate cancer. If true, the patient could become eligible for a drug called Olaparib, and it would then become imperative to test his 15-year-old daughter too. We collected patient’s blood and tested for BRCA and BRCAness genes. Indeed the patient came positive for BRCA mutation. While it brought cheer to him, he also got concerned for his daughter. We tested the daughter and several of his “at risk” first and second-degree relatives. While his daughter had no pathogenic BRCA mutation, and she was considered as normal as any individual, patient’s 30 years old sister was detected positive with the same BRCA mutation. Thus the clinical doctor has kept her on active surveillance while doing periodic mammogram and breast exams.
What are the things to keep in mind while opting for genetic testing? What are its hope for medical science in the days to come?
While opting for genetic testing, one should know that either the blood or tissue sample would be asked from the patient. I would advice patients to collect their tissue samples from pathology labs if ever their biopsy is done. Usually the tests takes more than ten days to give out the results. Patients should take time to understand their report from the treating doctor and, if necessary, call the molecular pathologist. The patient should provide the detailed family history to the genetic counsellors.
The genetic basis of most complex diseases is being identified every passing day. Identifying the genetic cause helps to detect “at risk family members” and helps find newer therapies for the patient to manage disease such as cancer.
What are the diseases for which it works?
Most inherited disorders such as Down’s syndrome, thalassemia/haemophilia, muscle dystrophy/spinal muscular atrophy can be detected using genetic testing. Genetic testing is also used in prenatal diagnosis, recurrent abortions, infertility, mental retardation. In complex diseases such as cancers, genomic testing can diagnose and give newer and better treatment options. Approximately, 6,000 genes are known to cause human disorders, and the same can be tested via different genetic tests. The rapid rate of gene discovery is increasing the number of diseases known on an almost daily basis.
Writer-filmmaker was in conversation with senior journalist Kaveree Bamzai at the launch of his novel Oonga at the recently concluded 14th edition of the Jaipur Literature Festival.
Sanjoy Roy: Welcome back to the 14th Jaipur Literature Festival protected by Dettol. We are delighted to bring it to you from here at the Diggi Palace front lawn live. It’s a pleasure to present today, Oonga by Devashish Makhija. He’s in conversation with Kaveree Bamzai and introduced by Nandita Das. Director and writer Devashish Makhija’s latest book Oonga is a powerful novel based on his first feature film of the same name. Capturing the inherent paradox between dystopian development and utopian ideologies, the book narrates the journey of a little boy in the midst of a clash between the Adivasis, the Naxalites, the CRPF and the mining company. Makhija’s other books include When Ali Became Bajrang Bali, Why Paploo Was Perplexed, Forgetting and Occupying Silence. He’s also the director of the feature films – Ajji and Bhonsle – and the short film Taandav. Among others, in his conversation with Kaveree Bamzai, Makhija dives into this evocative tale of identity and the tragedy of victims of violence forced into battles, they don’t wish to fight. The book is being launched here at the Jaipur Literature Festival 2021. Nandita Das has acted in more than 40 feature films in 10 different languages. Manto, Nandita’s second directorial film, premiered in 2018 at the Cannes Film Festival. Her first book, Manto and I, chronicles her six-year-long journey of making the film. Nandita, we’re delighted to have you here to make an introductory comment on Oonga, a film that you acted in. Nandita Das, over to you.
Nandita Das:Oonga is a film that I did almost nine years ago. When Dev came to me, it was his first film but I could see he was very passionate about the story and it’s a story that you know is really exploring the difficulties that Adivasis feel, especially as this is set in Odisha, a state that I come from, because they are caught between the Maoists, Naxal movements and outfits that are really fighting for their rights but can also get violent and at the same time those were trying to mainstream them in the name of development and how the common Adivasis just get completely caught between fighting for their rights and really not knowing how they should be dealing with their lives. You know, it’s a very complex issue and seldom do we see such complexities being told simply and powerfully. In fact, increasingly such films that are really representing stories of the people at large are vanishing from our collective consciousness. So it was definitely a film that I felt, I wanted to be part of. Hemla’s character was also really nice. It was very interesting because she’s kind of a conduit. She’s neither part of the Naxalite movement nor is she part of obviously the government or the mining corporation and all those people who are trying to mainstream them. She is really wanting to educate the children. She feels that’s where the power is and ideologically she’s very strong and it was lovely to be in Odisha and to be playing a character there. So yes, I mean it was a film that was close to my heart and I was really disappointed that it didn’t get released properly. Many independent films, unfortunately, bear with that fate.
I’m so happy that Dev decided to give it another form because the story had to be told and it’s really wonderful that now it’s in a book and we can all read it. And I think, you know, a story has its own soul and it must continue whether it’s through a film or through a book and maybe they’ll feed into each other. Maybe once you read the book, you’d want to see the film and those who have seen the film would want to read the book.
Nandita Das
Nandita Das introducing Oonga, the film, and Oonga, the novel.
I just want to wish Dev and the publishers and everyone who’s been involved with the project good luck, and I’m sorry that I couldn’t be at Diggi Palace, quite a favorite place to come to JLF, but here is wishing the book and the people who have been with that journey for this long. Twelve years is not a short journey. So glad Dev, that you stuck with it and that you’re bringing this story to us. Thank you!
Sanjoy Roy: Thank you, Nandita Das for setting the context for Oonga, the film and Oonga, the book.
Devashish Makhija has researched and assisted on the movies Black Friday and Bunty Aur Babli. He has written numerous screenplays, notably Anurag Kashyap’s yet-to-be-made superhero saga Doga, has had a solo art show Occupying Silence, written a collection of short stories Forgetting, the forthcoming book of poems Disengaged, the bestselling children’s books When Ali Became Bajrangbali and Why Paploo Was Perplexed and been featured in numerous anthologies including Mumbai Noir, Penguin First Proof and the Sahitya Akademi’s Modern English Poetry.
He has also written and directed the multiple award-winning short films Taandav, El’ayichi, Agli Baar, Rahim Murge Pe Mat Ro (Don’t Cry for Rahim LeCock), Absent, Happy, and the critically acclaimed full-length feature films Ajji (Granny) and Bhonsle. His films have competed and won awards at the international film festivals of Rotterdam, Gothenberg, Beaune, Black Nights, Busan, Glasgow, Tampere, MOMA, APSA, Barcelona, Singapore, amongst many others. Oonga, a feature film he wrote and directed in 2013 never released in Indian theatres despite a critically acclaimed film festival run so he reverse-adapted it into a gripping novel.
Kaveree Bamzai is an independent journalist. She was the first, and so far, only woman editor of India Today. A recipient of the Chevening Scholarship, she worked for the Times of India and Indian Express before this. She is the author of No Regrets: The Guilt-Free Woman’s Guide to a Good Life, Bollywood Today and two monographs in the series Women in Indian Film. She sits on several committees, including the Women Examplar Committee of CII and is recognised as a changemaker by Save The Children charity.
Kaveree: Devashish, it’s such a pleasure to see you and it’s been an absolute joy to read the book. I’ve spent the last two days doing that and it is truly gripping. It’s very powerful. I want to start with the line that you have there… “We, who take from the Earth and give back, will be replaced by those who take and never give back.” This really is who we are right now and I think the pandemic has taught us more than ever that this cannot go on. How amazing is it that the movie that you made, well, quite a few years ago, 2013, when it was released, is still so relevant? How amazing is that and how much more relevant is it? So, talk a little about that journey about making that movie, making this book and, at this moment in time.
Devashish: The sad thing is I don’t think it’s amazing as much as it’s hugely tragic. Yes, it’s hugely tragic that we can just never learn from our mistakes and I have travelled the areas, the Adivasi areas of Chhattisgarh and south Odisha about 11 years ago and for about five or six years before that, I was curious and dissatisfied with the narrative that I was reading in the mainstream media about what the Naxalites wanted; how they were being called to be the greatest internal security threat to this country by the Manmohan Singh Government and I felt that I wasn’t getting the complete picture. So when I travelled to those areas and the things that I saw, they sort of reeked of what the British had done to the Indians in all those years and now we were doing to our own countrymen. So, somewhere you know, that, that wheel was turning over and over again and we were not learning from our mistakes. What was relevant 200 years ago, was relevant 10 years ago. What was relevant 10 years ago, continues to be relevant today. I don’t know if it’s going to change. That’s the biggest heartbreaker.
So all the things that I wrote in Oonga in 2012 when I wrote the script and eight years hence when we were doing the final edits of the book, Tulika and I and I were re-reading material, re-reading my research (I had several exercise books where I had made notes as I was travelling through those areas), nothing had changed. Not one shred of research material or statistic or you know things that broke my heart in 2010. Nothing had changed. So somewhere, a book like this, sadly, would probably be relevant till we die.
Devashish Makhija
I don’t know what our next generation will see but the pandemic also hasn’t changed anything. We are back to being monsters. I thought we would, you know, re-evaluate our decisions, but no, we’re not.
Kaveree: Absolutely! And, in fact, Devashish, you also call it the company and company could be, you know, the company that you mentioned in the book. It could be the East India Company; really nothing changes; that’s really as you said is quite tragic.
The other point is the relationship between the Adivasis and their land and you know, we see it again and again and all the protests that we see — the farmers’ protests as well, their relationship with the land is so deep. And in fact, the land, and as you say in your book also reacts to their moods, you know, the trees cry, you know, the Earth cries; talk a little about that relationship. It’s so deep and so moving.
Devashish: Yeah. So in fact, it’s not just the Adivasis. If I say, any of us say that the Adivasis have this deep connection with nature and you know, we shouldn’t deprive them of that connection with nature. I think it will smack of an over-simplification. It will smack of talking about them as the other. I think we all have that connection; it’s just that with urban life, the kind of life that we live, we’re getting increasingly disconnected. So for me talking about these things using the Adivasi as a medium, was trying to tell urban youngsters, you know because it is young adult fiction; it’s for age group 16 and plus; I am hoping kids just out of school or in the last years of school will read this and wonder if they lost something by being born into these urbane, consumerist technologically, dependent lifestyles. So it’s all of us, who can, you know, pick cues from nature, live in harmony with nature and gain a lot, but we’ve just, we have lost that ability. So the Adivasis are a reminder that we have that ability and if we don’t live that codependent lives we are going to self-destruct faster and faster.
Kaveree: Yeah, another remarkable thing about the book is the women and I think that is the key here. The women are the ones who’re holding this community. They’re holding really a whole world aloft on their shoulders, you know, whether it’s Hemla or Oonga’s mother, they really are the spine, the backbone of the community.
Devashish: Women as characters and again I might smack of over-simplification here, but being a man when I made this film, Ajji, about five years ago, it was me trying to understand, what is the female energy and what is my relationship as a man being born into a world that is increasingly patriarchal. Even the MeToo movement really didn’t find success because we are so deep-rootedly patriarchal people; we need something stronger than that. So, from Ajji onwards, I’ve been questioning my role in the scheme of things that how can I raise questions that can hopefully someday 10 years or 100 years later lead to an answer.
The women that you speak of in Oonga, were there in the film as well. But I think I was not equipped to explore them to a certain depth like I could in the novel. For me Lakshmi, the Naxalite leader, Hemla and Oongamma are the beating heart of the story; Oonga is literally just the face. He’s not the beating heart of the story.
Devashish Makhija
So for me, it was important to explore those themes that I have now, you know been exploring the last four to five years. They were not in the film when we did that all those years back.
Kaveree: Devashish, the other thing is that it’s in Odisha, but it could be anywhere; it could be Kashmir, it could be the Northeast, that is the tragedy of India. It could be in any part of the country and it would be the same issue and I really admire the way you’ve been able to capture the CRPF sort of mindset, you know, it’s a very peculiar mindset, but we often don’t see them as victims and here you’ve been very non-judgmental and you have shown, they’ve suffered too. You have Pradip’s character, who realizes that the only way to have powers is to be in uniform; his father ended up in uniform guarding the very land that he sold them and it’s all such a terribly vicious cycle, but they are as well as victims.
Devashish: You know, as you were saying, it was a faceless company. It could be the East India Company. It could be a private company. It could be a public sector company. It was irrelevant to me what the company was. What was relevant to me was the thought process behind something as hegemonious and huge as a company that will only see its profit and when something that huge, you collectively are up against something, everybody ends up being a victim.
Sometimes even you don’t realize you’re a victim like Manoranjan, the CRPF commander. He doesn’t realize he’s a victim of a larger thought process, of a larger machine that is only using him for a certain end goal; and when you’re collectively up against that what can you be but a victim because you can’t use your mind and your consciousness to take decisions against that larger vicious thing; so for me, it was important to see that the CRPF are not in control. The Naxalites are reacting; they might have sometimes very very valid agenda, but they are not in control either.
Everybody is merely reactive and somewhere, the atmosphere that we live in today in this country, anyone who wants to question anything that the establishment does, we are all just reacting and that’s exhausting. I wish people act upon something sometimes because we spend all our lives we have reacting and we have no energy left to really act upon you know, our true impulses; somewhere that helplessness that I was feeling, I wanted to explore through this idea of everyone being a victim; a helpless victim.
Devashish Makhija
Oonga, reverse adapted from a critically acclaimed film.
Kaveree: Absolutely. I think, the other point that every form of protest that we see, every form of dissent that we see, you see echoes of it in your book. The idea of asking for papers. The idea of asking for identity. I mean the whole agitation against CAA was all about that. The whole question is being explored here. It is quite contemporary in that sense. Talk a little about that sense of identity as well. The Adivasi sense of identity versus the Company, which could be anything. How does it play out?
Devashish: You have to look at the farmers’ protest today. When I speak to my peers, my contemporaries in the city, everyone looks at the farmers of India as one big mass. A faceless mass. And when they talk about what they’re up against, the government policies which are pro-corporate, you have an Adani or Ambani which has a face. They are not faceless.
Somewhere those who don’t understand what the farmers are protesting for and if they don’t try to understand how that’s important to the rest of us. We will always see that protesters faceless and they will always see what they’re protesting against as having a face and that’s what makes it easier for them to relate to you know the system because the system always comes with some sort of a face, be it the government or a corporate. So here also in my story, I was trying to flip it. I was trying to make the company faceless. I was trying to give a sense of identity to those who are paying that price, whether it was the CRPF or the Adivasi. It could be the farmers today in India or it could be the Dalit.
Devashish Makhija
It could be you know for lack of a better metaphor here, I myself feel rather displaced because I’m a Sindhi. My parents both of them came from Pakistan, which is now Pakistan during the partition. I was born and I grew up in Calcutta where I wasn’t a Bengali, but I was around Bengali culture a lot. I’ve been working in Bombay for 18 years, but I’m not Marathi, but I’m around Marathi culture a lot. My two films are Ajji and Bhonsle and, if you don’t know better, sound like Marathi films so I have been struggling with identity. I don’t know where my roots are. Yeah, so when I am trying to question the system as to my place in the scheme of things, I don’t know where to begin because I have nothing to prove that I have an identity that allows me to question this system.
If I multiply my helplessness by 5,000, I get the helplessness of an Adivasi or a Dalit or a farmer and for me, that breaks my heart, so I needed to give them faces and explore their identity.
Kaveree: The other interesting thing in the story is the importance of the eye. You see it everywhere in the novel. Everyone has to keep an eye out, ahead, behind. There is a symbol of the eye that represents the company. I found that again a very very powerful metaphor. Talk about that.
Devashish: Again you have beautifully caught it because somewhere I was trying to simplify and allegorise the idea of surveillance and today with modern technology, the system can observe you, surveil you a lot more but it’s always been the case. Even when we had landline phones, if the government wanted, they could tap your line. This goes back to my research for Black Friday. I spent six months researching material that S. Hussain Zaidi had already put in the book, but when you try to give faces for cinema, you need to research the people a little more deeply. So around that time, I spoke to people whom I can’t name. I spoke to the CBI. I spoke to people in the IB. I spoke to the police, the crime branch and there were thousands of hours of phone recordings that they had of people that I can’t name, but they’re like all the phones were tapped and they were just surveilling, surveilling, surveilling, all the time. I asked them that you know, you’ve got all this material, what is that you want to do with it. They said, if we release or leak it, we will not be able to hold on to the government for more than five minutes. So they sit on all this material.
I knew that back to the 1960s, when we could tap anything anywhere at will; today it has just become easier. So how do you then live a life of Liberty, Equality, Fraternity and all the things that the Constitution enshrines? How do you live that life? If you are being watched all the time? If you are supposed to toe the line. Do you walk the talk that the system wants you to? How do you manifest those ideas in the Constitution? So that idea of the eye for me was to create that sense of dread that you know, you’re being watched and you don’t have freedom even though you think that you do. It is a delusion.
Devashish Makhija
Kaveree: Yeah, absolutely, but I found in Hemla’s character so much purity, so much courage and so much fearlessness and I think that is the fearlessness that we have lost as a society. We’re also afraid. Aren’t we? I think that’s the biggest threat to us. It’s not what the state is doing to us. It’s not what the environment is doing to us and it’s our own fear and I think Hemla is such a hero to me because she has so much courage.
Devashish: One of my biggest inspirations for Hemla was Soni Sori and when I sort of knew more about her or watched her at work. There’s a line that I use often that a woman without hope is a woman without fear. So when you take away hope and I saw it in Soni Sori’s eye. If you look into her eyes, I see an absence of Hope, but that doesn’t mean that it manifests as utter Hopelessness. The absence of Hope is not Hopelessness but that absence of hope because she seemed so much taken away brings her certain courage. She has nothing left to lose. What do you take away from her anymore? So somewhere for Hemla, I wanted to manifest that she might have seen so much that we are not privy to that she cannot fear anymore. What is the worst that can happen that she will be physically assaulted, that someone will chop her hands off? She has seen that too. She has seen that happen. And something a friend of mine said to me during those journeys through the Adivasi area. He said that you know, we have to lose our fear of being thrown in jail.
Most of the time people don’t act upon a certain thing that they want to question the government about because they are afraid that they will get thrown in jail. He said you have to obliterate that fear. Forget that you will die in jail. You will get food. You will be able to take a piss when you want. You will get to dump once a day. You will get to sleep. Maybe the mosquitoes would bother you, but you will not die in jail. So if you take away that fear, it takes away your fear to question the system because the system has only one way to bring you down. By disciplining you. By throwing you in jail. By threatening you with a warrant. So I want to take talk about those things through Hemla.
Devashish Makhija
Kaveree: And you have done that really well. The other point I think comes through so powerfully is that question that we saw of the huge exodus during the pandemic when people went home and they were walking the streets with all their belongings on them. It’s not just about poverty. I think at the end of the day, it is about dignity. They want respect and if you don’t give it to them then, you know, at some point they will break.
Devashish: Dignity is everything and that’s one of the saddest things when you go to an Adivasi village where maybe five or six men have been missing for years because they were thrown in jail for merely asking for their rights. The first thing you see is that crushed soul because amongst themselves there’s a lot of dignity, but when they have to face the system like we went on to help one of the Praja lawyers there with a particular bunch of cases. So because we could read and write in English, so it was easier to read documents for them. These documents come by the fucking kilogram, so they always need help to read documents and respond to them. So we went to jail and we tried talking to the Jailor. We tried talking to their lawyer the first thing that the Jailor or the lawyer did was to get up and look through us and walk away. We felt insulted. Now imagine, we were there for a month and a half. Now imagine having to put up with that every day where you’re not acknowledged. When nobody looks you in the eye. Nobody talks to you. They just get up and walk away. That can make you think of doing very extreme things.
Kaveree: And yet you have Hemla trying her best to initiate dialogue, trying the best to teach Hindi to children so that they can grow up and speak to the company or the CRPF or whoever in their own language. So there is some amount of hope but it gets crushed so easily. Yet that plea for peaceful dialogue is still a very powerful hope that you end with even in your book, although it is dystopian. It is still there. The plea for hope. The plea for dialogue. To understand each other and to listen to each other. Let’s talk a little about how that is so much an absence, not just in that community, but everywhere, currently.
Devashish: You know that the dystopia that you speak of I think manifests in that one line wherein the end Hemla has run back to the Village. She still trying to talk to Manoranjan, but suddenly she has this gun pointed in her face and she suddenly realizes that I’ve been talking to the barrel of this gun all the time. I’ve not been talking to the people behind it because this is what they thrust in my face when I’m actually pleading. Somewhere that absence of communication that everyone is talking different languages.
When I say different languages, I don’t mean literally someone speaking Kovi or someone speaking Hindi but someone speaking the language of the gun when someone’s trying to speak the language of the heart. There cannot be a dialogue in such a situation. The gun has to be put down if there has to be a dialogue. When you see the farmers’ protests, there are water cannons or tear gas, metal rods. When you walk in with that you can’t have a dialogue with farmers who actually didn’t want to attack you in the first place and they still haven’t. But the face of the system is always, almost always, that of, you know of a violent weapon and you cannot talk to that beyond a point. The weapon has to be shed. Faces have to emerge for that dialogue to happen and somewhere the book is trying to entreaties. It is trying to make a case for that. But how possible is it until that effort is taken from both sides, not just one side?
Devashish Makhija
Kaveree: What does it do to you personally? You see all these beautiful, proud people, as you said earlier, you see their souls being crushed and you see so much oppression. I mean we see it too, but you’ve undertaken this journey and you have chronicled it. What does it do to you as a person?
Devashish: I had behavioural issues around the time I was working on this material. I’ve had physiological issues. Around the time I was making Ajji, I contracted prostate cancer and I didn’t realize then why these things were happening. But when you’re experiencing this and I’m not as strong as Medha Patkar. I don’t have those qualities to shield myself, to keep myself disaffected to carry on the fight because I’m always trying to take that emotion and create something of it. When I’m channelling that emotion through me, it is leaving something in me. So I had to grapple with my own demons that sort of got created when I see what I see or when I interact with the people I do and hopefully I try and manifest all of that into my story so that they don’t stay within me entirely, but of course, they don’t entirely go away either. So I have a life of stories inside me that have to do with all of this material. So a lot of my peers ask me, “Don’t you want to make a happy story? Don’t you want to tell a love story? The biggest tragedy is that I have love stories inside me. I have mainstream ideas. I have happy stories. I don’t have the opportunity to say them because there’s so much else. I finish with the Adivasi struggle and there’s the Dalit who needs representation. You finish with that and then there is patriarchy. You finish with that and then there is something else. The country is tearing at its seams with how horrific we are in the way we treat our own countrymen.
Kaveree: I mean I come from a state which has become a complete mental asylum. It’s an open mental asylum. Kashmir, I think is the most paranoid state in this country because it’s been like this now for over 25 years. They’ve lived with this surveillance thing. But the whole idea of nature feeling us. When you talk about the trees and the grass, they feel for us. They soak it all in, you know, when the Adivasis talk about the strange view that has come and they talk about nature feeling their pain. How much of that do you think is happening around us. You know, when we look at the raging environmental crisis. Is that nature’s way of feeding off some toxicity in a way?
Devashish: How can nature escape that if we are such an intrinsic part of nature. Say about a thousand years or 2,000 years back, we were not the most proliferating species on this planet. So there were other species maybe. Maybe they were more rats than human beings 2,000 years ago. So nature still has some chance of staying balanced, but now there are so many of us and we also emerged from nature. So when we are going to go around destroying what we ourselves a part of, will there not be a backlash? And I think, it is getting exponentially exacerbated. I think what we are thinking global warming might destroy us by 2055. It might happen by 2028 because it’s just exponentially getting worse. We are and we have been proliferating like a virus. Maybe COVID is one way of nature trying to find the little balance. I’m surprised that we had COVID so light. Like I thought we’d have it much worse.
Writer-filmmaker Devashish Makhija in coversation with senior journalist Kaveree Bamzai about his novel Oonga at the recently concluded Jaipur Literature Festival 2021.
Kaveree: Yeah, and I don’t think it’s changed us too much fundamentally. The other opposition I see so starkly in the novel is between Lakshmi and Hemla. It’s not just the ideology of the gun versus education, but it’s also the idea of giving in to your anger and I think that again is one of the greatest tragedies of our time. We have given in to our anger; we’ve given in it to our rage. Hemla is still someone who tries not to do that, but Lakshmi is too far gone on that path again. This is such a fundamental contrast.
Devashish: Oh, yes. So unfortunately when I started writing Oonga many years ago, I wanted to give Hemla some sort of a culmination in hope because I believe in her stance but as the story progressed, more and more, it felt too me that Laksmi is right and Hemla is being foolish and somewhere by the end, I couldn’t control it. It just went out of control and Laxmi survives and Hemla pays the price for believing.
Kaveree: That’s really tragic. But unfortunately, it’s the truth.
Devashish: Yes, I don’t know. Given the current climate.
Kaveree: More than ever.
Devashish: Punning on the word climate, I think across the world. I don’t know how we can escape this tragedy unless we all start thinking, you know, positively all at once, and believe in the right things, all at once. It can’t happen piecemeal anymore.
Kaveree: Another interesting thing that I found in your book is reclaiming of Ram by Oonga. I found that lovely because here you have Ram who’s been appropriated as a symbol by a very toxic movement and here you have this little boy, sort of appropriating Ram in the purest way possible, and in the sweetest way possible. This is something quite remarkable. And I think this is something again that you must talk a bit about this little boy believing in Ram and believing that he can vanquish Ravan.
Devashish: So now at the expense of probably calling a fatwa on my head by the very frightening right-wing. So on 6 December 1992. I’ll just take a minute to trace this back to an experience, a very personal experience. On 6 December 1992, in a little mohalla in Calcutta, I was 12-13 and we were one of three Hindu families in a predominantly Bangladeshi Muslim slum. The news of the masjid being demolished reaches this mohalla and we were attacked that night. My mother was almost raped. And that never left me. I didn’t feel anger for whoever was attacking us as more as much as I felt confusion. I didn’t know why that happened. The next morning. We were almost back to normal because I had to go buy eggs from a shop in the slum. I had to you know, navigate those same gullies that I was navigating every day growing up in that Mohalla so that stayed with me and somewhere every time someone says that there is a bhoomi where Ram was born, I have a physical response to that because you can’t literalise a metaphor. Ram is a metaphor for you know, certain values. All the characters of the Ramayana or the Mahabharata stand for certain values. Storytelling back then and even today is literally about dispensing values to the people you are telling those stories to through the characters that you populate those stories with.
So Oonga is my Ramayana, my Mahabharata, my modern mythology through which I’m trying to impart certain values. So for me to put forth that idea that Ram was, stood or represented certain ideas and was not real, was the most important thing for me in this story because it sort of achieves many things at many levels. It achieves that the idea that he goes beyond religion. So Ram is not just a Hindu metaphor anymore. Ram could be an Adivasi. He could be that Adivasi who stood up for his jungle and didn’t want his jungle destroyed by the industry and when little Oonga, a 10-11-year-old boy will actually arrive at the heart of that metaphor much quicker than an adult because he doesn’t have those trappings and those conditionings that adults do. So he finds the heart of Rama being an Adivasi and much quicker.
Devashish Makhija
He arrives at the metaphor and therefore when he understands at a very subconscious level that this is a metaphor so if Ram is a metaphor then what’s stopping me from being Ram and I can replicate those values and those ideas where I come from. So I want to send out this messaging because the right-wing has appropriated from me the things that I took away from the Ramayana, so this is me trying to take it back.
Kaveree: You do it really well, Devashish. I wanted to know what makes you? What keeps you going?
Devashish: One thing that also breaks me is the one thing that keeps me going. There is an unending abyss of rage. I try not showing it half the time when I’m constantly grappling with it, trying to subdue it, trying to therapeutise it, but when I sit down and tell a story, I dip into that rage. Without that rage, I don’t know how to tell stories. So it’s rage all the way. I would rather it come into my stories then manifest in me picking up the gun.
Kaveree: I really want to ask what’s next for you?
Devashish: Like I was telling Sanjoy earlier, all my stories are really hard to find backing for so I am trying. I’ve got like 15-16 stories that I’m trying to turn into films, but I’m hoping that this novel does well. The films I make get watched by a very niche audience. They almost never make their money back. So it takes me three-four years to set up a film so somewhere, you know, a storyteller like me is not getting the energy back that I’m putting into the world. So I’m hoping this book finds readers so that I feel like I’ve been energized enough. I would actually drop everything and write my next novel which is ready. And it has all the same motifs that Oonga did, only that they are a lot more personal. It’s about that night on the 6th of December 1992 in that mohalla in Kolkata.
To buy the book, click here.
(The above text – transcription and editing – is a handiwork of Suman Bhattacharya and Shillpi A Singh)
On World Oral Health Day 2021, Dr Hitesh R Singhavi tells us why oral hygiene is a must.
New Delhi, March 20, 2021: Did you know that people whose inner cheek, teeth and gums are in poor condition may be more susceptible to mouth and throat cancers? Well, here is what you should know. Oral cancer is one of India’s most common cancers amongst men (11.28% of all cancers), the fifth most frequently occurring cancer amongst women (4.3% of all cancers). The causes attributed to oral cancer are mainly tobacco chewing, areca nut, alcohol consumption, and poor oral hygiene (POH). We often associate poor oral hygiene with dental caries, Gingivitis, Periodontitis (gum disease) and foul smell. Still, poor oral hygiene, in the long run, can give rise to fatal diseases, including cancer. A British study has shown that patients with poor oral health index have an overall higher mortality rate (they die prematurely) compared to others. Let’s take a look at the frequently asked question related to poor oral hygiene and oral cancer.
WHAT ARE THE FACTORS CAUSING POOR ORAL HYGIENE? There are numerous common factors leading to poor oral hygiene, including tobacco chewing, alcohol, areca nut chewing, infrequent dental visits, immunocompromised status, low socio-economic status, and lower education level. Studies have shown that all these factors significantly deteriorate oral hygiene.
HOW DOES POOR ORAL HYGIENE CAUSE ORAL CANCER? POH is strongly associated with oral cancers. It aids the carcinogenic potential of other known carcinogens, like tobacco and alcohol. It causes easy conversion (faster endogenous nitration) of tobacco metabolite into cancer causing products (nitrosamines), leading to cancer development. POH also reacts with alcohol to form Aldehyde-also a class I carcinogen (Class I carcinogen are the product which can independently cause cancer).
HOW CAN YOU PREVENT ORAL CANCER BY MAINTAINING GOOD ORAL HYGIENE? One should not consume tobacco or tobacco products, which is one of Gingival Recession’s major causes (loss of gums), leading to loosening of teeth and the formation of a pre-cancerous lesion. Similarly, avoiding alcohol consumption may help maintain good oral hygiene, as evidence shows that an alcohol consumer has higher chances of foul-smelling mouth, more tar burdened teeth, and a greater possibility of bleeding gums.
WHICH ARE THE PARTS OF ORAL CAVITY YOU SHOULD LOOK FOR CANCEROUS LESION ASSOCIATED WITH POOR ORAL HYGIENE? Buccal Mucosa (inner cheek mucosa) is the most common oral cavity cancer site when POH is associated with tobacco chewing habit. When POH is associated with alcohol, then under the tongue’s surface, the floor of the mouth is the most common site.
CAN SHARP TOOTH OR ILL-FITTING DENTURE CAUSE ORAL CANCER? Chronic mucosal trauma due to a sharp tooth or ill-fitting dentures can cause oral cancer. A study conducted by Tata Memorial Centre (Singhavi et al) has concluded that chronic mucosa trauma has higher chances of developing oral cancer. It’s not an uncommon finding to have oral cancer in non-habitual patients, especially tongue cancers. Chronic mucosa trauma and poor oral hygiene are the front runners in such cases.
Evidence that ascertains the link between poor oral hygiene and oral cancer: Level 1 (direct causation) evidence to determine poor oral hygiene as the primary etiological factor of oral cancer is lacking. However, studies have shown that maintaining good hygiene reduces the chances of oral cancer by 200%. Also, 93 relevant articles published in the literature until the year 2020 concluded that poor oral hygiene contributes to oral cancer causation, in one way or the other. However, for more information, refer to https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6414580.
Thus, on the occasion of World Oral Health Day, which is observed on March 20th, 2021, let’s pledge to spread the word and educate people on the significance of oral health and sensitise people that maintaining good oral hygiene is a must to stay away from oral cancer.
(Dr Hitesh R Singhavi is Consultant, Head and Neck Surgeon, Fortis Hospital, Mulund; Image by Daniel Albany from Pixabay)